Short anagen syndrome
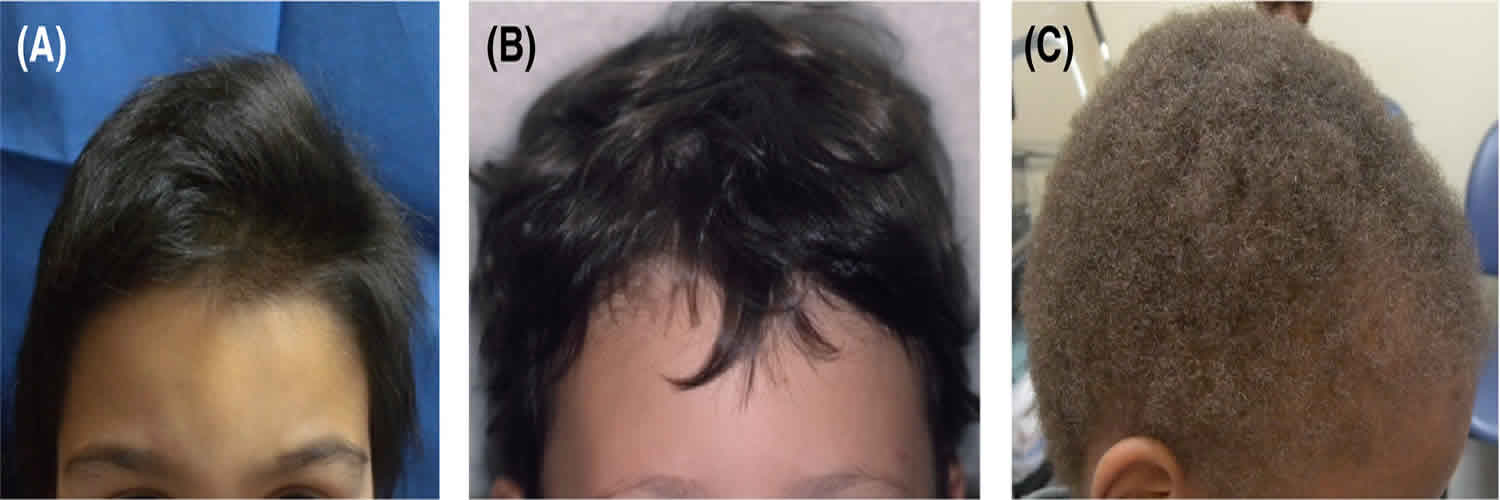
Short anagen syndrome or short anagen hair syndrome, is a harmless and rare congenital (present at birth) hair condition in which hair does not grow long 1. Short anagen syndrome is a benign disease of the hair cycle. Short anagen syndrome is clinically characterized by persistently short fine hair since birth, due to a decreased duration of the anagen phase 2. Anagen is the growing phase of the normal hair cycle and is followed by telogen – the hair sheds or moults during telogen (see Figure 3 below). Another anagen hair then starts to grow in the same follicle. In short anagen syndrome, the duration of anagen may be only a year or two, compared to the normal 4 to 7 years. It usually presents in childhood, with parents reporting that their child ‘can’t grow their hair long’ or has ‘never had a haircut’. Short anagen syndrome is usually perceived by parents in children around 2-4 years of age.
The common complaint is that the hair does not grow long 3 and that it has never been cut 4. Telogen effluvium which is a temporary hair loss due to the excessive shedding of resting or telogen hair after some shock to the system, is also a common complaint. Only a few cases have been published in the literature, mainly in Caucasian blond-haired girls 4. Although some authors claim that short anagen is rare 5, others believe that it is just under-recognized 3.
Short anagen syndrome is unassociated with hair breakage, total hair loss, and any other serious association 5. Short anagen syndrome differential diagnosis is loose anagen syndrome, which is a hair disorder characterized by anagen hairs of abnormal morphology that are easily and painlessly pulled or plucked from the scalp. Loose anagen syndrome hair is thinned in appearance and typically does not grow beyond the nape of the neck.
How does your hair grow?
Hair is a slender filament of keratinized cells that grows from an oblique tube in the skin called a hair follicle. Each hair is composed of columns of dead, keratinized epidermal cells bonded together by extracellular proteins. The hair shaft is the superficial portion of the hair, which projects above the surface of the skin. The hair root is the portion of the hair deep to the shaft that penetrates into the dermis, and sometimes into the subcutaneous layer.
Hairs project beyond the surface of the skin almost everywhere except the sides and soles of the feet, the palms of the hands, the sides of the fingers and toes, the lips, and portions of the external genitalia. There are about 5 million hairs on the human body, and 98 percent of them are on the general body surface, not the head. Hairs are nonliving structures that form in organs called hair follicles.
The density of hair does not differ much from one person to another or even between the sexes; indeed, it is virtually the same in humans, chimpanzees, and gorillas. Differences in apparent hairiness are due mainly to differences in texture and pigmentation.
Types of hairs
Hairs first appear after about three months of embryonic development. These hairs, collectively known as lanugo, are extremely fine and unpigmented. Most lanugo hairs are shed before birth.
The two types of hairs in the adult skin are vellus hairs and terminal hairs:
- Vellus hairs are the fine “peach fuzz” hairs found over much of the body surface.
- Terminal hairs are heavy, more deeply pigmented, and sometimes curly. The hairs on your head, including your eyebrows and eyelashes, are terminal hairs. After puberty, it also forms the armpit and pubic hair, male facial hair, and some of the hair on the trunk and limbs.
Hair follicles may alter the structure of the hairs they produce in response to circulating hormones.
Figure 1. Hair structure
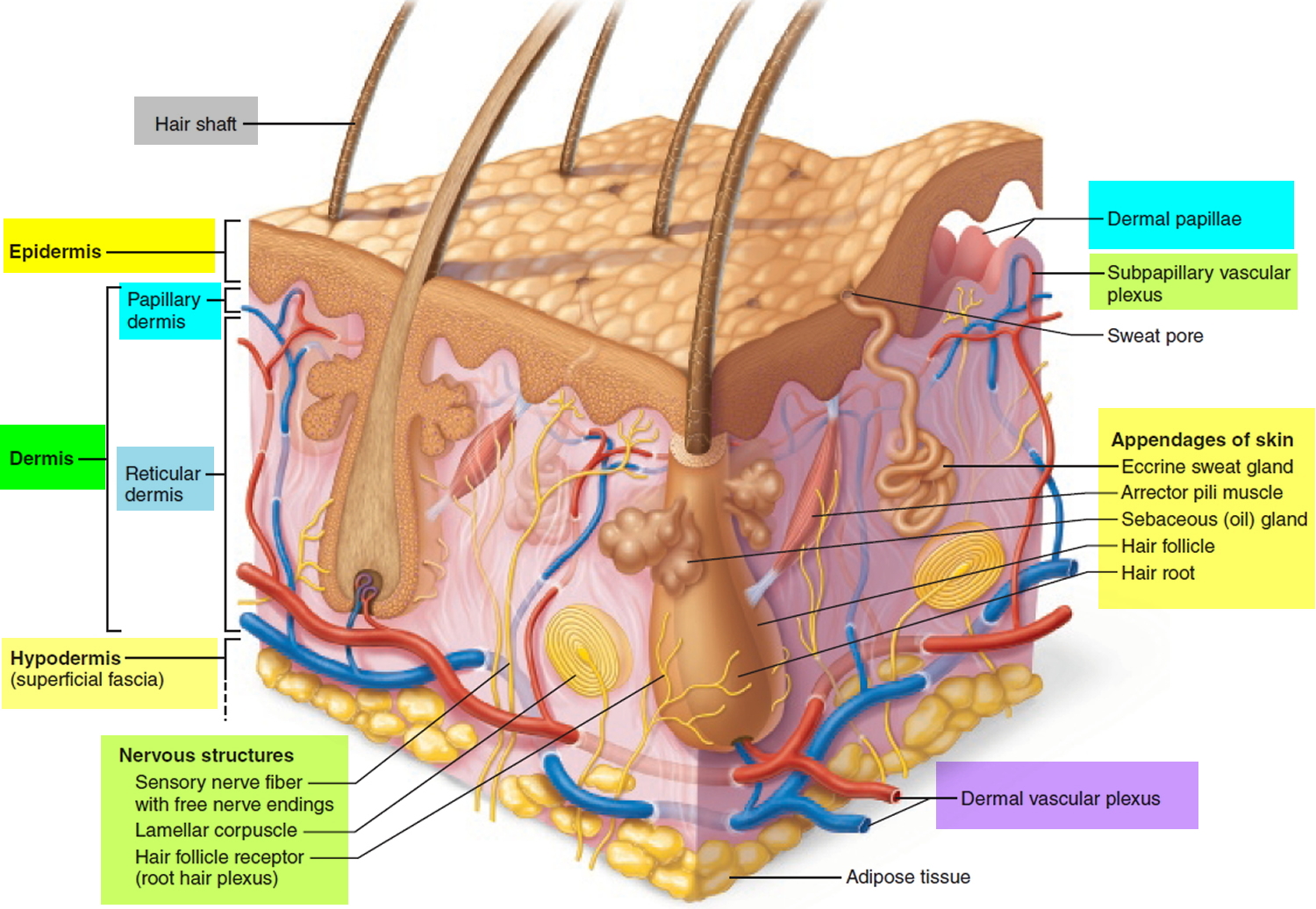
Figure 2. Hair follicle
Hair production
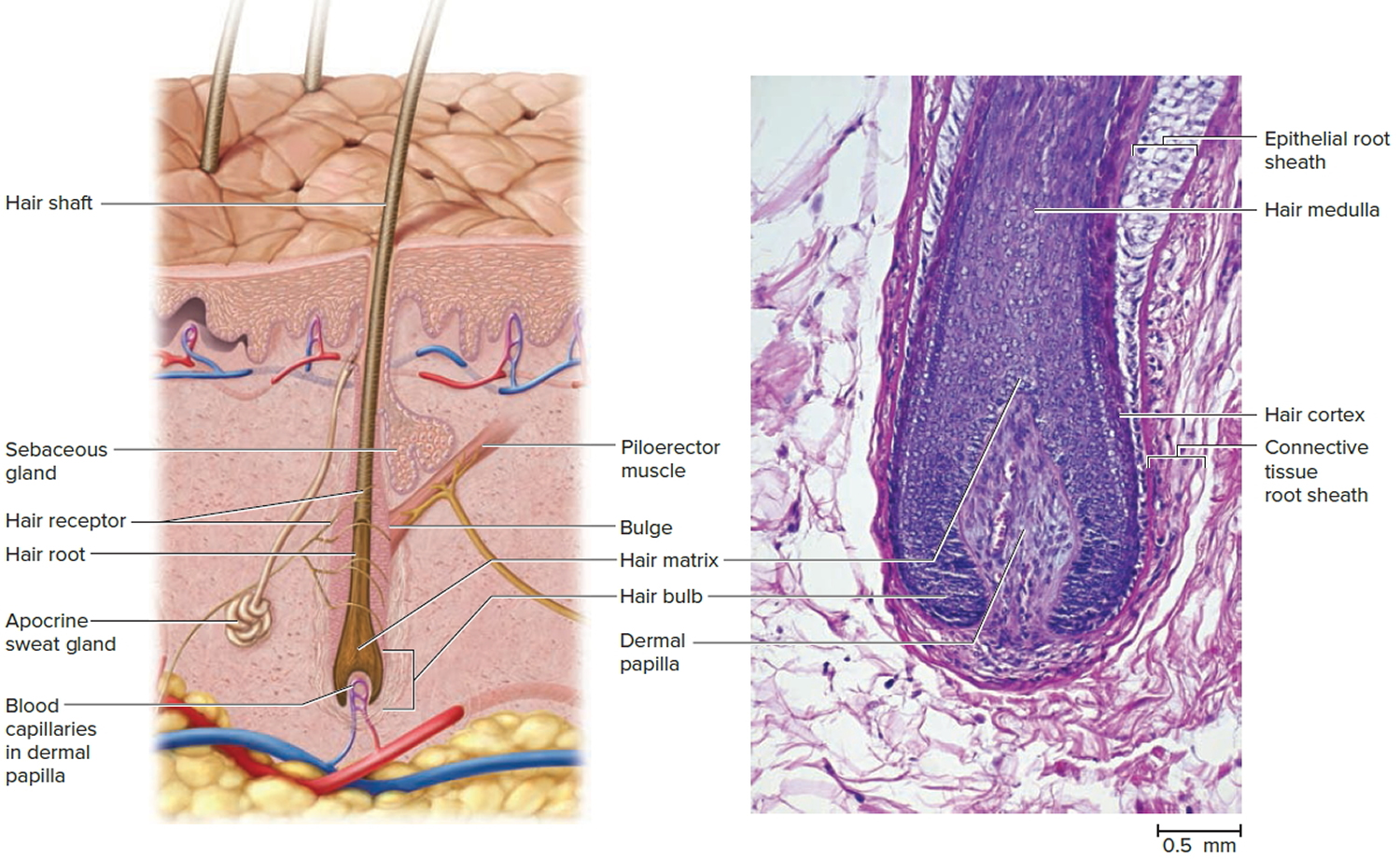
Hair follicles extend deep into the dermis, often projecting into the underlying subcutaneous layer. The epithelium at the follicle base surrounds a small hair papilla, a peg of connective tissue containing capillaries and nerves. The hair bulb consists of epithelial cells that surround the papilla.
Hair production involves a specialized keratinization process. The hair matrix is the epithelial layer involved in hair production. When the superficial basal cells divide, they produce daughter cells that are pushed toward the surface as part of the developing hair. Most hairs have an inner medulla and an outer cortex. The medulla contains relatively soft and flexible soft keratin. Matrix cells closer to the edge of the developing hair form the relatively hard cortex. The cortex contains
hard keratin, which gives hair its stiffness. A single layer of dead, keratinized cells at the outer surface of the hair overlap and form the cuticle that coats the hair.
The hair root anchors the hair into the skin. The root begins at the hair bulb and extends distally to the point where the internal organization of the hair is complete, about halfway to the skin surface. The hair shaft extends from this halfway point to the skin surface, where we see the exposed hair tip.
The size, shape, and color of the hair shaft are highly variable.
Growth and Replacement of Hair
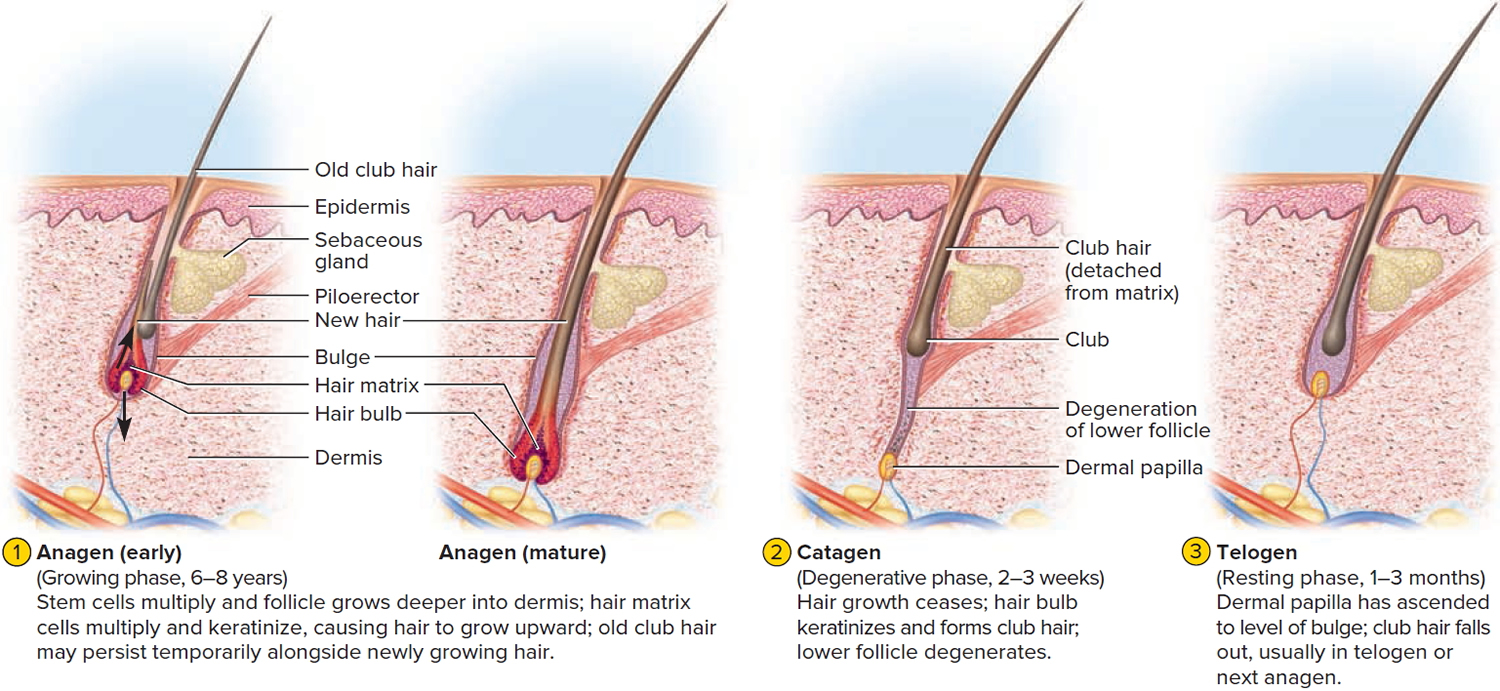
A hair in the scalp grows for two to five years, at a rate of around 0.33 mm/day (about 1/64 inch). Variations in hair growth rate and the duration of the hair growth cycle account for individual differences in uncut hair length. A given hair goes through a hair cycle consisting of three developmental stages (see Figure 3):
- Anagen.
- Catagen.
- Telogen.
At any given time, about 90% of the scalp follicles are in the anagen stage. In this stage, stem cells from the bulge in the follicle multiply and travel downward, pushing the dermal papilla deeper into the skin and forming the epithelial root sheath. Root sheath cells directly above the papilla form the hair matrix. Here, sheath cells transform into hair cells, which synthesize keratin and then die as they are pushed upward away from the papilla. The new hair grows up the follicle, often alongside an old club hair left from the previous cycle.
In the catagen stage, mitosis in the hair matrix ceases and sheath cells below the bulge die. The follicle shrinks and the dermal papilla draws up toward the bulge. The base of the hair keratinizes into a hard club and the hair, now known as a club hair, loses its anchorage. Club hairs are easily pulled out by brushing the hair, and the hard club can be felt at the hair’s end. When the papilla reaches the bulge, the hair goes into a resting period called the telogen stage. Eventually, anagen begins anew and the cycle repeats itself. A club hair may fall out during catagen or telogen, or as it is pushed out by the new hair in the next anagen phase.
You lose about 50 to 100 scalp hairs daily. In a young adult, scalp follicles typically spend 6 to 8 years in anagen, 2 to 3 weeks in catagen, and 1 to 3 months in telogen. Scalp hairs grow at a rate of about 1 mm per 3 days (10–18 cm/yr) in the anagen phase.
Hair grows fastest from adolescence until the 40s. After that, an increasing percentage of follicles are in the catagen and telogen phases rather than the growing anagen phase. Hair follicles also shrink and begin producing wispy vellus hairs instead of thicker terminal hairs. Thinning of the hair, or baldness, is called alopecia. It occurs to some degree in both sexes and may be worsened by disease, poor nutrition, fever, emotional stress, radiation, or chemotherapy. In the great majority of cases, however, it is simply a matter of aging.
Pattern baldness is the condition in which hair is lost unevenly across the scalp rather than thinning uniformly. It results from a combination of genetic and hormonal influences. The relevant gene has two alleles: one for uniform hair growth and a baldness allele for patchy hair growth. The baldness allele is dominant in males and is expressed only in the presence of the high level of testosterone characteristic of men. In men who are either heterozygous or homozygous for the baldness allele, testosterone causes terminal hair to be replaced by vellus hair, beginning on top of the head and later the sides. In women, the baldness allele is recessive. Homozygous dominant and heterozygous women show normal hair distribution; only homozygous recessive women are at risk of pattern baldness. Even then, they exhibit the trait only if their testosterone levels are abnormally high for a woman (for example, because of a tumor of the adrenal gland, a woman’s principal source of testosterone). Such characteristics in which an allele is dominant in one sex and recessive in the other are called sex-influenced traits.
Excessive or undesirable hairiness in areas that are not usually hairy, especially in women and children, is called hirsutism. It tends to run in families and usually results from either masculinizing ovarian tumors or hypersecretion of testosterone by the adrenal cortex. It is often associated with menopause.
Contrary to popular misconceptions, hair and nails do not continue to grow after a person dies, cutting hair does not make it grow faster or thicker, and emotional stress cannot make the hair turn white overnight.
Figure 3. Hair growth cycle
Short anagen syndrome causes
The cause of short anagen syndrome is unknown. Most reported cases have occurred in single members of a family and so far no genetic abnormality has been found 6. Short anagen syndrome was first described in 1991 and there are few case reports 7.
Short anagen syndrome is usually benign, nevertheless associations with tricho-dental syndrome 8, synchronized pattern of scalp hair growth 9 and micronychia 2 have been reported.
Short anagen syndrome signs and symptoms
Short anagen syndrome usually presents in childhood, with parents reporting that their child ‘can’t grow their hair long’ or has ‘never had a haircut’. Short anagen syndrome is usually perceived by parents in children around 2-4 years of age. The common complaint is that the hair does not grow long 3 and that it has never been cut 4.
Short anagen syndrome diagnosis
In short anagen syndrome, the hair shaft is otherwise normal, apart from its length. The density of the hair is normal, the hairs are not fragile, and they do not break easily. The diagnosis of short anagen hair syndrome can be made by presence of normal hair shafts, unbroken hair, and decreased number of hair in anagen 4. The characteristic clinical image and the finding of short (less than 6 cm long) telogen hairs with a tipped point at the pull test or trichogram makes the diagnosis 3. Short anagen syndrome must be differentiated from other conditions causing short hair.
The hair pull test is often normal. This test is conducted by grasping and then gently pulling on a group of 20 to 50 scalp hairs. The number of hairs that can easily be extracted is normally around 2 to 10, mainly telogen hairs. A normal result in short anagen syndrome helps differentiate it from loose anagen syndrome, in which many more hairs than normal are extracted, or other hair shedding syndromes such as telogen effluvium, which will have a higher percentage of telogen (bulb) hairs.
The rest of the physical examination is normal without any abnormalities in skin, teeth or nails. Children with short anagen syndrome have normal mental and physical development.
Investigations may include:
- Dermoscopic examination of the scalp hair density
- Microscopic examination of hair shafts
- Hair pull test (described above)
- Scalp biopsy
Short anagen syndrome treatment
Treatment is not necessary as this condition tends to improve after puberty 3, however improvement with minoxidil and cyclosporine has been reported 2.
Minoxidil 5% solution applied twice daily is believed to stimulate hair follicles to enter into anagen and prolong the duration of anagen. However, its efficacy has not been well established in the treatment of short anagen syndrome.
Minoxidil solution dilates small blood vessels. When applied to the affected areas of the scalp twice daily it has been shown to stimulate hair regrowth probably by enhancing cell proliferation. It is possible it also has an effect on the immune cells in the hair follicle.
Most reported cases of short anagen syndrome have persisted to adulthood. This is in contrast to loose anagen syndrome, which improves with age.
Further research is needed to establish diagnostic criteria and better treatment modalities for short anagen syndrome.
References- Herskovitz I, de Sousa IC, Simon J, Tosti A. Short anagen hair syndrome. Int J Trichology. 2013;5(1):45-46. doi:10.4103/0974-7753.114711 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746230
- Jung HD, Kim JE, Kang H. Short anagen syndrome successfully controlled with topical minoxidil and systemic cyclosporine A combination therapy. J Dermatol. 2011;38:1108–10.
- Giacomini F, Starace M, Tosti A. Short anagen syndrome. Pediatr Dermatol. 2011;28:133–4.
- Avashia N, Woolery-Lloyd H, Tosti A, Romanelli P. Short anagen syndrome in an African American woman. J Am Acad Dermatol. 2010;63:1092–3.
- Antaya RJ, Sideridou E, Olsen EA. Short anagen syndrome. J Am Acad Dermatol. 2005;53:S130–4.
- Avashia N, Woolery-Lloyd H, Tosti A, Romanelli P. Short anagen syndrome in an African American woman. J Am Acad Dermatol. 2010. May 21. [Epub ahead of print]
- Giacomini F, Starace M, Tosti A. Short Anagen Syndrome. Pediatr Dermatol. 2010. Jun 9. [Epub ahead of print]
- Kersey PJ. Tricho-dental syndrome: A disorder with a short hair cycle. Br J Dermatol. 1987;116:259–63.
- Thai KE, Sinclair RD. Short anagen hair with persistent synchronized pattern of scalp hair growth. J Am Acad Dermatol. 2003;49:949–51.





{kind=link}