What is situs inversus
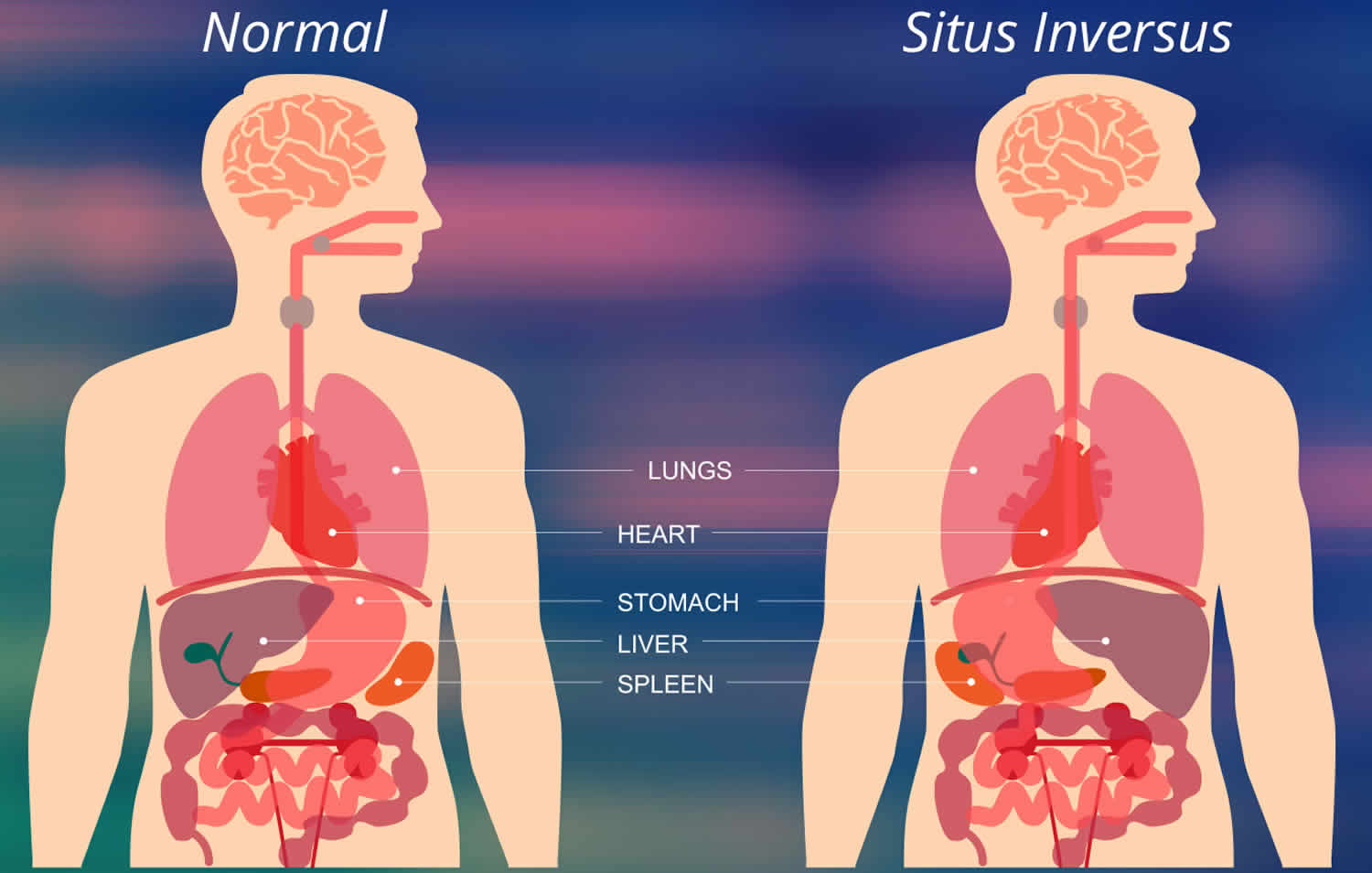
Situs inversus is short form of the Latin words “situs inversus viscerum” or situs transversus, is a rare condition (1 in 8,500 people) causing inverted position of chest and abdominal organs 1. It is called situs inversus totalis when there is a total transposition of abdominal and thoracic viscera (mirror image of internal organs normal positioning). Many people with situs inversus are asymptomatic of their unusual anatomy until they are evaluated medically for unrelated conditions 2 or diagnosed incidentally during laparotomy or autopsy 3. But, when associated with midgut volvulus or atresias, it would present early in the neonatal age 4. The normal anatomical position of internal organs is termed as situs solitus 5.
Situs inversus abdominus also known as situs inversus with levocardia or left-located heart is a condition with right-to-left reversal limited to the abdomen 6. In situs inversus totalis, there is complete right to left reversal of all of the viscera including dextrocardia; the morphologic right atrium is on the left and the left atrium is on the right. The normal pulmonary anatomy is reversed such that the left lung has three lobes and the right lung has two. The liver and gallbladder are located on the left, and spleen and stomach are on the right side 7. Associated anomalies with situs anomaly are congenital heart disease or splenic malformations 3.
Situs inversus is usually associated with dextrocardia (true mirror image) with only 3-5% incidence of congenital heart disease, most commonly transposition of the great vessels. Of these patients, 80% have a right-sided aortic arch. Situs inversus with levocardia (which is much rarer: 0.00005%) congenital heart disease is found in 95% of patients 8.
Up to 20% of patients with situs inversus can have Kartagener syndrome 9 which comprises a subgroup of primary ciliary dyskinesia.
Situs inversus imaging features on chest radiograph to be evaluated are:
- location of heart apex
- location of aortic arch
- location of stomach bubble / liver
Situs inversus occurs more commonly with dextrocardia 10. A 3-5% incidence of congenital heart disease is observed in situs inversus with dextrocardia, usually with transposition of the great vessels. Of these patients, 80% have a right-sided aortic arch. Situs inversus with levocardia is rare 11 and it is almost always associated with congenital heart disease 12.
The typical clinical phenotype of primary ciliary dyskinesia includes any or all of the following: neonatal respiratory distress; chronic, persistent lower respiratory symptoms (early onset and persistent wet cough); chronic, persistent upper respiratory symptoms (nasal congestion and otitis media), and a laterality defect (situs inversus or ambiguous). The presence of any 2 of these features provides a strong clinical phenotype for primary ciliary dyskinesia. At least 12% of primary ciliary dyskinesia patients have situs ambiguous, and these patients have a 200-fold increased probability of having structural congenital heart disease as compared to the general population with heterotaxy 13.
The recognition of situs inversus is important for preventing surgical mishaps that result from the failure to recognize reversed anatomy or an atypical history. For example, in a patient with situs inversus, cholecystitis typically causes left upper quadrant pain, and appendicitis causes left lower quadrant pain. A trauma patient with evidence of external trauma over the ninth to eleventh ribs on the right side is at risk for splenic injury 14. If surgery is planned on the basis of radiographic findings in a patient with situs inversus, the surgeon should pay careful attention to image labeling to avoid errors such as a right thoracotomy for a left lung nodule.
Figure 1. Situs inversus with dextrocardia
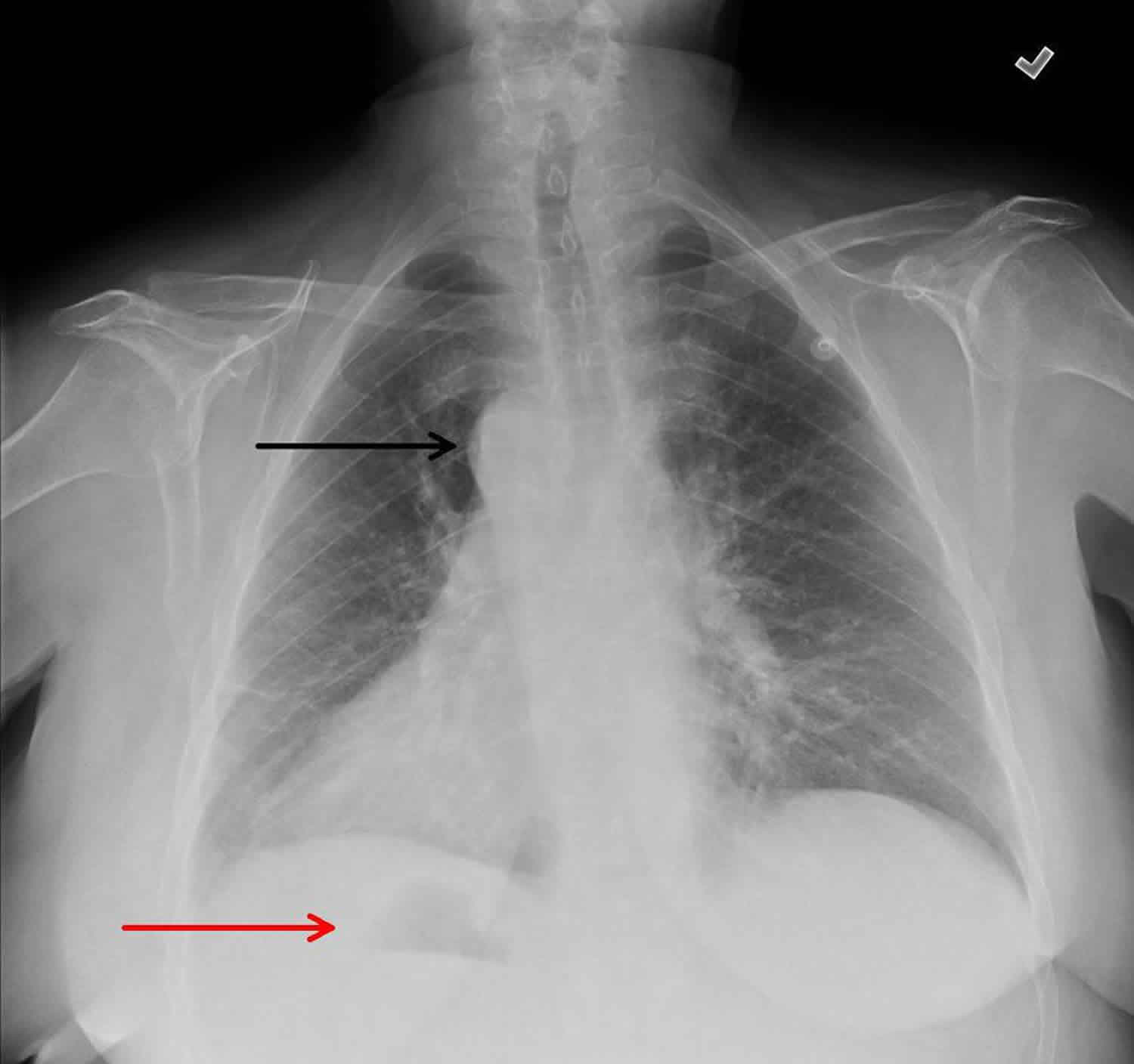
Footnote: Frontal radiograph reveals situs inversus. Right aortic arch (black arrow), dextrocardia, and right-sided stomach bubble (red arrow). Note that the image has been labeled correctly and is not flipped.
Types of situs inversus
Situs inversus can be classified further into situs inversus with levocardia and situs inversus with dextrocardia. The classification of situs is independent of the cardiac apical position. The terms levocardia and dextrocardia indicate only the direction of the cardiac apex at birth; they do not imply the orientation of the cardiac chambers. In levocardia, the base-to-apex axis points to the left, and in dextrocardia, the axis is reversed. Isolated dextrocardia is also termed situs solitus with dextrocardia. The cardiac apex points to the right, but the viscera are otherwise in their usual positions. Situs inversus with dextrocardia is also termed situs inversus totalis because the cardiac position, as well as the atrial chambers and abdominal viscera, is a mirror image of the normal anatomy. Situs inversus totalis has an incidence of 1 in 8,000 births. Situs inversus with levocardia is less common, with an incidence of 1 in 22,000 births 15.
When situs cannot be determined, the patient has situs ambiguous or heterotaxy. In these patients, the liver may be midline, the spleen absent or multiple, the atrial morphology unclear, and the bowel malrotated. Often, normally unilateral structures are duplicated or absent. The 2 primary subtypes of situs ambiguous include (1) right isomerism, or asplenia syndrome, and (2) left isomerism, or polysplenia syndrome. Heterotaxy syndromes have an incidence of 1 in 10,000 newborn births but account for about 4% of all congenital heart disease 15.
In classic right isomerism, or asplenia, bilateral right-sidedness occurs. These patients have bilateral right atria, a centrally located liver, and an absent spleen, and both lungs have 3 lobes. The descending aorta and inferior vena cava are on the same side of the spine. Right isomerism has an incidence of between 1 in 10,000 and 1 in 20,000 births, male predominance, and a nearly 100% incidence of congenital heart disease. It often presents in childhood with a cyanotic heart defect such as a common AV canal, univentricular heart, transposition of the great arteries, or total anomalous pulmonary venous return 15.
In left isomerism, or polysplenia, bilateral left-sidedness occurs. These patients have bilateral left atria and multiple spleens, and both lungs have 2 lobes. Interruption of the inferior vena cava with azygous or hemiazygous continuation is often present. Left isomerism has an incidence of between 1 in 10,000 and 1 in 20,000 births and a female predominance. Associated cardiac malformations include partial anomalous pulmonary venous return, atrial septal defect (ASD), and a common atrioventricular (AV) canal 15.
The features of situs ambiguous are inconsistent; therefore, situs ambiguous cases are challenging and require thorough evaluation of the viscera 16. The location and relationships of the following should be reviewed carefully: abdominal viscera, hepatic veins, superior vena cava, inferior vena cava, coronary sinus, pulmonary veins, cardiac atria, atrioventricular connections and valves, cardiac ventricles, position of the cardiac apex, and aortic arch and great vessels.
Situs inversus causes
The underlying cause and genetics of situs inversus are complex. Several familial cases have been reported in which the inheritance has been described as either autosomal recessive (most commonly), autosomal dominant, or X-linked 17. Situs inversus appears to be genetically heterogeneous, meaning that different genetic factors or genes may cause the condition among different people or families. If situs inversus is associated with another underlying syndrome or condition, the inheritance pattern may be the same as that of the underlying condition.
People with questions about genetic risks to themselves or family members are encouraged to speak with a genetics professional.
Situs inversus symptoms
In isolated situs inversus (occurring alone with no other abnormalities), there is a complete mirror image transposition of the thoracic (chest) and abdominal organs, and anterior-posterior (front-back) symmetry is normal. Many affected people have no associated health issues when the condition is isolated. When situs inversus occurs in association with other conditions such as Kartagener syndrome or primary ciliary dyskinesia, additional signs and symptoms relating to these conditions will be present 18.
Situs inversus diagnosis
A thorough physical examination, followed by radiographic imaging of the chest and abdomen and electrocardiography, identify most cases of situs inversus. The main diagnostic challenge in affected people is the non-traditional presence of referred pain (pain felt in a different location than its source) 18.
Situs abnormalities may be recognized first by using radiography or ultrasonography 19. However, computed tomography (CT) scanning is the preferred examination for the definitive diagnosis of situs inversus with dextrocardia. CT scanning provides good anatomic detail for confirming visceral organ position, cardiac apical position, and great vessel branching. Magnetic resonance imaging (MRI) is usually reserved for difficult cases or for patients with associated cardiac anomalies 20. Most patients with situs inversus with levocardia require additional imaging to evaluate the associated cardiac anomalies. When radiation exposure is a concern, MRI or ultrasonography may be preferred.
The differential diagnosis includes appendicitis, asplenia/polysplenia, congenital coronary abnormalities, sinusitis, and ventricular septal defect. Other conditions to be considered are primary ciliary dyskinesia, heterotaxy, left isomerism (ie, Ivemark syndrome), right isomerism (ie, asplenia syndrome), situs solitus, and transposition of the great arteries.
If radiologic intervention is to be performed in a patient with situs inversus, the condition should be known from earlier diagnostic imaging. A question of improper image labeling must be resolved before any procedure is initiated 21. Failure to recognize situs inversus before performing a radiologic procedure may result in intervention on the incorrect side of the patient. Attention to the left and right sides of the patient and the left and right labeling of images is helpful to prevent mistakes in diagnosis and/or surgical intervention.
Discordance between the direction of the cardiac apex and the abdominal situs suggests congenital heart disease. Situs ambiguous and situs inversus with levocardia have this discordance between the direction of the cardiac apex and the abdominal situs; thus, further imaging is usually needed.
Situs inversus treatment
In isolated situs inversus, no treatment may be necessary. When situs inversus is associated with another condition, treatment may depend on the associated condition and the signs and symptoms present in the affected person 18.
Knowing that a person has situs inversus is important for diagnosing medical problems and preventing surgical mishaps that can result from the failure to recognize reversed anatomy. For example, in a person with situs inversus, appendicitis causes pain in the left lower abdomen instead of the right lower abdomen 22. Wearing medical identification can help ensure proper treatment in an emergency medical situation.
Situs inversus prognosis
The long-term outlook (prognosis) for people with situs inversus depends on whether the condition is isolated, or is associated additional abnormalities affecting the heart or other parts of the body. Isolated situs inversus has an excellent prognosis, typically with an uneventful prenatal and postnatal course 23. When situs inversus is associated with an underlying condition or syndrome, the prognosis may depend on that of the underlying condition present.
For fetuses diagnosed with situs inversus on prenatal ultrasound, additional testing such as fetal MRI and fetal echocardiography may provide additional information about the development of the fetus, which may affect management and prognosis 24. Additional imaging tests are also recommended after birth to further clarify any associated abnormalities that may be present. People who learn of a diagnosis made by prenatal ultrasound are encouraged to meet with a genetic counselor or other genetics professional.
Knowing that a person has situs inversus is important for diagnosing medical problems and preventing surgical mishaps that can result from the failure to recognize reversed anatomy. For example, in a person with situs inversus, appendicitis causes pain in the left lower abdomen instead of the right lower abdomen 22. Wearing medical identification can help ensure proper treatment in an emergency medical situation.
Situs inversus life expectancy
In most cases, affected individuals can live a normal life without any symptoms or discomfort. If situs inversus is associated with other more serious heart malformations, the prognosis and treatment will vary.
References- Genetics of human situs abnormalities. Casey B. Am J Med Genet. 2001 Jul 15; 101(4):356-8. https://www.ncbi.nlm.nih.gov/pubmed/11471159
- Gupta R, Soni V, Valse PD, Goyal RB, Gupta AK, Mathur P. Neonatal intestinal obstruction associated with situs inversus totalis: two case reports and a review of the literature. J Med Case Rep. 2017;11(1):264. Published 2017 Sep 18. doi:10.1186/s13256-017-1423-z https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5603179
- Nawaz A, Matta H, Hamchou M, Jacobez A, Trad O, Al Salem AH. Situs inversus abdominus in association with congenital duodenal obstruction: a report of two cases and review of the literature. Pediatr Surg Int. 2005;21:589–92. doi: 10.1007/s00383-005-1412-y
- Sharma S, Rashid KA, Dube R, Malik GK, Tandon RK. Congenital duodenal obstruction with situs inversus totalis: report of a rare association and discussion. J Indian Assoc Pediatr Surg. 2008;13(2):77–8. doi: 10.4103/0971-9261.43029
- Clinical aspects of defects in the determination of laterality. Aylsworth AS. Am J Med Genet. 2001 Jul 15; 101(4):345-55.
- Abdur-Rahman LO, Adeniran JO, Taiwo JO. Concurrent dextrogastria, reverse midgut rotation and intestinal atresia in a neonate. J Indian Assoc Pediatr Surg. 2007;12(4):228–30. doi: 10.4103/0971-9261.40843
- Ekpe EE, Uwah U, Nyong EE. Dextrocardia with situs inversus co-existing with neonatal intestinal obstruction. Port Harcourt Med J. 2008;2(2):177–80. doi: 10.4314/phmedj.v2i2.38919
- Oski’s pediatrics. LWW. ISBN:0781738946
- Applegate KE, Goske MJ, Pierce G et-al. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 19 (4): 837-52
- Maldjian PD, Saric M. Approach to dextrocardia in adults: review. AJR Am J Roentgenol. 2007 Jun. 188(6 suppl):S39-49; quiz S35-8.
- Gindes L, Hegesh J, Barkai G, Jacobson JM, Achiron R. Isolated levocardia: prenatal diagnosis, clinical importance, and literature review. J Ultrasound Med. 2007 Mar. 26(3):361-5.
- Xu BP, Shen KL, Hu YH, Feng XL, Li HM, Lang ZQ. [Clinical characteristics of primary ciliary dyskinesia in children]. Zhonghua Er Ke Za Zhi. 2008 Aug. 46(8):618-22
- Knowles MR, Zariwala M, Leigh M. Primary Ciliary Dyskinesia. Clin Chest Med. 2016 Sep. 37 (3):449-61.
- Liu Y, Wu L, Chen Y, Li D, Jiang J, Zhong W, et al. Delayed diagnosis of abdominal pain in patient with situs inversus totalis in emergency department: A case report. Medicine (Baltimore). 2017 Dec. 96 (49):e9028
- Mujo T, Finnegan T, Joshi J, Wilcoxen KA, Reed JC. Situs ambiguous, levocardia, right sided stomach, obstructing duodenal web, and intestinal nonrotation: a case report. J Radiol Case Rep. 2015 Feb. 9 (2):16-23
- Lee SE, Kim HY, Jung SE, et al. Situs anomalies and gastrointestinal abnormalities. J Pediatr Surg. 2006 Jul. 41(7):1237-42
- Talabi AO, Sowande OA, Tanimola AG, Adejuyigbe O. Situs inversus in association with duodenal atresia. Afr J Paediatr Surg. July-September, 2013; 10(3):275-278. https://www.ncbi.nlm.nih.gov/pubmed/24192475
- Dextrocardia with Situs Inversus. https://rarediseases.org/rare-diseases/dextrocardia-with-situs-inversus
- Kashiwagi S, Ishikawa T, Onoda N, Kawajiri H, Takashima T, Hirakawa K. Laparoscopic adrenalectomy in a patient with situs inversus. JSLS. 2013. 17(3):487-90.
- Boland MR, Lowery AJ, Walsh S, Beddy D, Prichard RS, O’Shea D, et al. Incidental Phaeochromocytoma on Staging PET-CT in a Patient with a Sigmoid Tumour and Situs Inversalis Totalis. Case Rep Surg. 2014. 2014:645462
- Sirin BH, Kurdal AT, Iskesen I. Congenitally corrected transposition of the great arteries plus dextrocardia operated with an unusual operative technique. Thorac Cardiovasc Surg. 2008 Sep. 56(6):367-9
- Situs Inversus Imaging. https://emedicine.medscape.com/article/413679-overview
- Alfred Z. Abuhamad, Rabih Chaoui. Fetal Heterotaxy, Left Atrial Isomerism, Right Atrial Isomerism, and Situs Inversus. A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Nemec SF, et. al. Situs anomalies on prenatal MRI. Eur J Radiol. April, 2012; 81(4):e495-501





{kind=link}