
What is tendinopathy
Tendinopathy is a broad term encompassing painful conditions occurring in and around tendons in response to overuse 1. Tendons are tough bands of tissue that connect muscles to bones. Repetitive activities and overuse can injure tendons, leading to pain and impaired function. This is called tendinopathy. Some people call this condition tendinitis, although the more correct term is tendinopathy because most people do not have inflammation 2. Recent basic science research suggests little or no inflammation is present in tendinopathy. Histopathologic changes associated with tendinopathy include degeneration and disorganization of collagen fibers, increased cellularity, and minimal inflammation 3. Macroscopic changes include tendon thickening, loss of mechanical properties, and pain 4. Recent work demonstrates several changes occuring in response to overuse including the production of matrix metalloproteinases, tendon cell apoptosis, chondroid metaplasia of the tendon, and expression of protective factors such as insulin-like growth factor 1 (IGF-1) and nitric oxide synthetase (NOS) 5. Although many of these biochemical changes are pathologic and result in tendon degeneration, others appear beneficial or protective 1. Tendinopathy appears to result from an imbalance between the protective/regenerative changes and the pathologic responses that result from tendon overuse. The net result is tendon degeneration, weakness, tearing, and pain 1.
Tendinopathy has a multifactorial cause: ageing, overuse, genetic, epigenetic, and inflammation all play roles in its course 2. Although the most common cause of tendinopathy is wear and tear over time, overuse can cause sudden swelling and tendinitis. It can also be caused by other conditions, including rheumatic diseases 6.
Tendinopathy is a common problem. The risk of developing tendinopathy increases with age and is higher in people who routinely perform activities that require repetitive activities in work or sport. Treatment focuses on resting the injured tendon to allow healing, using techniques to decrease pain, and exercising to improve muscle strength and tendon stability.
Tendon physiology
Tendons are composed of a highly organized structure to allow for the transmission of large-magnitude forces between muscle and bone during daily activities. The structure relies on highly regulated interplay between the activity of local cell types and the regulation of extracellular matrix composition (Figure 1). The extracellular matrix composition is composed of parallel collagen fibers that can be further divided into fascicles, fibrils, subfibrils, microfibrils, and tropocollagen components 7. Collectively, the bundled fibers are surrounded by connective tissue layers – epitenon and endotenon – that allow for frictionless movement and supply blood vessels, nerves, and lymphatics to deeper tendon structures. Regulation of this highly organized structure by tenocytes, tenoblasts, and tendon stem/progenitor cells (TSPCs) is crucial to maintain proper mechanical properties and prevent injury 8.
As tendons transmit forces between muscle and bone during repeated motion, they become susceptible to acute and chronic injury 9. There are many mechanisms of injury that lead to tendinopathy or tendon rupture, and the injury can be due to a combination of both acute and chronic trauma. For example, tendon ruptures may occur in the setting of acute overload or laceration, but are often secondary to intrinsic pathology 9. Participating in a sporting activity is the most common etiologic factor for Achilles tendon rupture, but biopsies have shown degenerative changes in most ruptured Achilles tendons 10. As such, this type of injury is classified by some authors as acute trauma of chronically degenerated tendons 9.
In addition to damage induced by stresses that are outside physiological limits, such as rupture or laceration, repetitive microtrauma that occurs within physiologic limits can induce tendinopathy and increase risk of acute and chronic injury. Repetitive loading can be detrimental to tendon structure, as the repair mechanism has less time to heal the microtrauma before subsequent stresses 11. Also, microtears can be induced by nonuniform force production and muscle activation that results in nonuniform loading of tendons. This indicates that both load magnitude and distribution are critical factors in the determination of tendon-injury etiology 11.
Several ideas have been proposed to underlie the etiology of tendinopathy, including hypoxia, ischemic damage, oxidative stress, induction of apoptosis, and production of inflammatory cytokines 12. For instance, following ischemia induced by maximal tensile load, relaxation and subsequent generation of free radicals may play a role in tendinopathy 12. Supporting this idea is the upregulation of peroxiredoxin 5, an antioxidant enzyme present in human tenocytes, in cases of tendinopathy 13. In addition, localized hypoxia may result in failure to maintain necessary ATP levels and contribute to degeneration 14.
It has also been demonstrated that strain application induces the production of protein kinases that regulate apoptosis of tenocytes 15. Furthermore, protein-kinase activity demonstrates a magnitude-dependent rather than frequency-dependent response. Animal models have shown that administration of harmful inflammatory mediators, such as prostaglandin E2 and IL6, induces tendinopathy histologically 16. Physiologic levels of cyclic stretching have also been shown to induce secretion of IL6 in tenocytes 17. Although the relative contribution of each of these biologic processes requires further investigation, tendinopathy is most likely due to a combination of these propositions. Although tendons have some regenerative capacity, their mechanical properties and highly ordered structural organization will not return to preinjury levels even after extended periods 18.
Figure 1. Tendon anatomy and structure
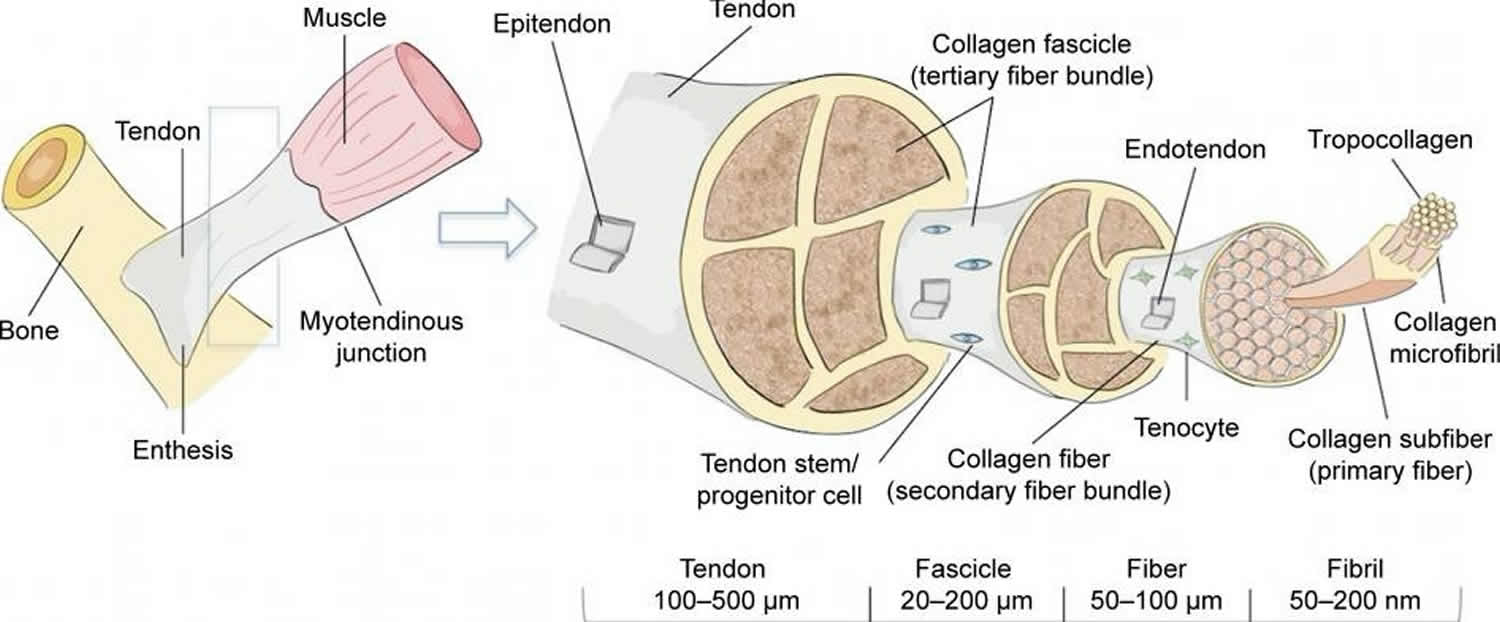
Footnote: Collagen alignment is based on organization into fascicles, fibers, and fibrils. Tenocytes, terminally differentiated from tenoblasts, are the main cellular component of tendons. Though the exact location of tendon stem cells is unknown, their presence has been confirmed. Blood vessels and nerves are also present within the structure, but are not shown.
[Source 19]Shoulder tendonitis
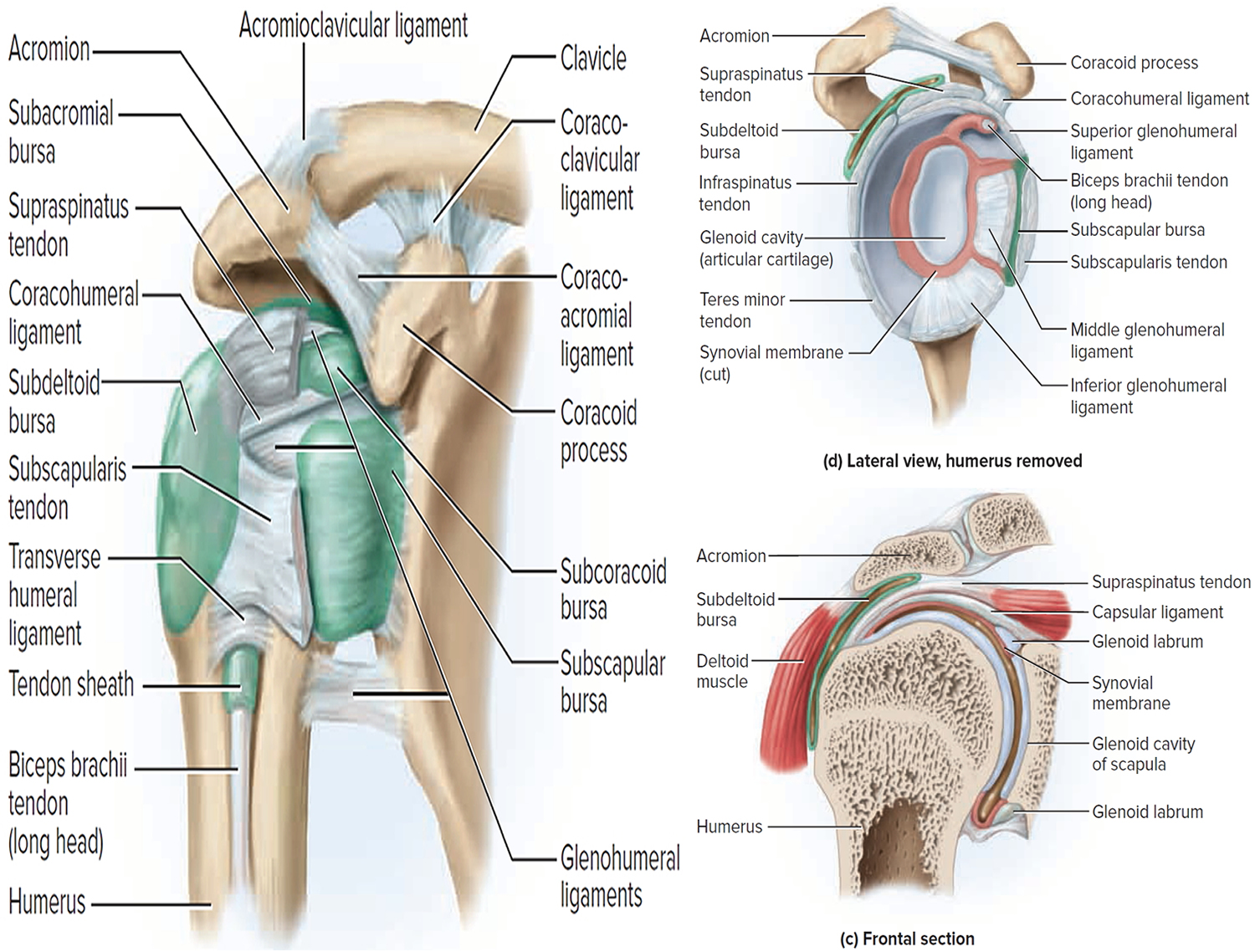
The main joint in the shoulder is formed by the arm bone and the shoulder blade. The joint socket is shallow, allowing a wide range of motion in the arm. The rotator cuff is made up of 4 muscles that surround the arm bone (see Figure 1). This cuff keeps the shoulder steady as the arm moves.
The supraspinatus muscle rests on top of the shoulder. Its tendon travels under the bone on the outside of the shoulder (the acromion). This tendon is the one most often injured because of its position between the bones. As the tendon becomes inflamed (sore and swollen), it can become pinched between the 2 bones. The sac of fluid that cushions the tendon can also be damaged.
A common cause of shoulder pain is soreness of the tendon (a cord that attaches a muscle to a bone) of the rotator cuff. This is the part of the shoulder that helps circular motion. Another common cause is soreness of the subacromial bursa (a sac of fluid under the highest part of the shoulder). You might experience soreness after painting, lifting items, or playing a sport—anything that requires you to lift your arms. Or you may not remember any specific injury, but you still feel pain in your shoulder.
The rotator cuff is a common source of pain in the shoulder and the pain can be the result of:
- Tendinitis. The rotator cuff tendons can be irritated or damaged.
- Bursitis. The bursa can become infl amed and swell with more fluid causing pain.
- Impingement. When you raise your arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or “impinge” on) the tendon and the bursa, causing irritation and pain.
Figure 2. Shoulder joint
Causes of shoulder tendonitis
Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible.
Pain may also develop as the result of a minor injury. Sometimes, it occurs with no apparent cause 20.
Symptoms of shoulder tendonitis
Rotator cuff pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position.
Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage.
These symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
Diagnosis of shoulder tendonitis
After discussing your symptoms and medical history, your doctor will examine your shoulder. He or she will check to see whether it is tender in any area or whether there is a deformity. To measure the range of motion of your shoulder, your doctor will have you move your arm in several different directions. He or she will also test your arm strength.
Your doctor will check for other problems with your shoulder joint. He or she may also examine your neck to make sure that the pain is not coming from a “pinched nerve,” and to rule out other conditions, such as arthritis.
Imaging Tests
Other tests which may help your doctor confirm your diagnosis include:
- X-rays. Because x-rays do not show the so tissues of your shoulder like the rotator cuff , plain x-rays of a shoulder with rotator cuff pain are usually normal or may show a small bone spur. A special x-ray view, called an “outlet view,” sometimes will show a small bone spur on the front edge of the acromion.
- Magnetic resonance imaging (MRI) and ultrasound. These studies can create better images of so tissues like the rotator cuff tendons. They can show fluid or
inflammation in the bursa and rotator cuff. In some cases, partial tearing of the rotator cuff will be seen.
Treatment for shoulder tendonitis
The goal of treatment is to reduce pain and restore function. In planning your treatment, your doctor will consider your age, activity level, and general health.
Nonsurgical Treatment
In most cases, initial treatment is nonsurgical. Although nonsurgical treatment may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest. Your doctor may suggest rest and activity modification, such as avoiding overhead activities.
Non-steroidal anti-inflammatory (NSAIDs) medicines. Drugs like ibuprofen and naproxen reduce pain and swelling.
Physical therapy. A physical therapist will initially focus on restoring normal motion to your shoulder. Stretching exercises to improve range of motion are very helpful. If you have difficulty reaching behind your back, you may have developed tightness of the posterior capsule of the shoulder (capsule refers to the inner lining of the shoulder and posterior refers to the back of the shoulder). Specific stretching of the posterior capsule can be very effective in relieving pain in the shoulder.
Once your pain is improving, your therapist can start you on a strengthening program for the rotator cuff muscles.
The following exercises may help you. Ask your doctor if you should do other exercises, too.
Range of motion
Stand up and lean over so you’re facing the floor. Let your sore arm dangle straight down. Draw circles in the air with your sore arm. Start with small circles, and then draw bigger ones. Repeat these exercises 5 to 10 times during the day. If you have pain, stop. You can try again later.
Rotator cuff strengthening
Use a piece of rubber tubing for these exercises. Stand next to a closed door with a doorknob. Loop the tubing around the knob. With your hand that is closest to the door, bend your arm at a 90° angle (at the elbow) and grab the loop of the tubing. Pull the band across your tummy. At first, do 1 set of 10 exercises. Try to increase the number of sets as your shoulder pain lessens. Do these exercises every day.
Upper extremity strengthening
As your pain goes away, try adding a general upper body weight-lifting program using weight machines or free weights. Lie on your right side with your left arm at your side. With a weight in your left hand and your forearm across your tummy, raise your forearm. Keep your elbow near your side.
Steroid injection. If rest, medications, and physical therapy do not relieve your pain, an injection of a local anesthetic and a cortisone preparation may be helpful. Cortisone is a very effective anti-inflammatory medicine. Injecting it into the bursa beneath the acromion can relieve pain.
Surgical Treatment for Shoulder Tendonitis
When nonsurgical treatment does not relieve pain, your doctor may recommend surgery.
The goal of surgery is to create more space for the rotator cuff. To do this, your doctor will remove the inflamed portion of the bursa. He or she may also perform
an anterior acromioplasty, in which part of the acromion is removed. This is also known as a subacromial decompression. These procedures can be performed using either an arthroscopic or open technique.
Arthroscopic technique
In arthroscopy, thin surgical instruments are inserted into two or three small puncture wounds around your shoulder. Your doctor examines your shoulder through a fiberoptic scope connected to a television camera. He or she guides the small instruments using a video monitor, and removes bone and so tissue. In most cases, the front edge of the acromion is removed along with some of the bursal tissue.
Your surgeon may also treat other conditions present in the shoulder at the time of surgery. These can include arthritis between the clavicle (collarbone) and the acromion (acromioclavicular arthritis), inflammation of the biceps tendon (biceps tendonitis), or a partial rotator cuff tear.
Open surgical technique
In open surgery, your doctor will make a small incision in the front of your shoulder. This allows your doctor to see the acromion and rotator cuff directly.
Rehabilitation
After surgery, your arm may be placed in a sling for a short period of time. This allows for early healing. As soon as your comfort allows, your doctor will remove the sling to begin exercise and use of the arm.
Your doctor will provide a rehabilitation program based on your needs and the findings at surgery. This will include exercises to regain range of motion of the shoulder and strength of the arm. It typically takes 2 to 4 months to achieve complete relief of pain, but it may take up to a year.
Elbow tendonitis
Tennis elbow or lateral epicondylitis, is a painful condition of the elbow caused by overuse 21. Not surprisingly, playing tennis or other racquet sports can cause this condition. However, several other sports and activities can also put you at risk.
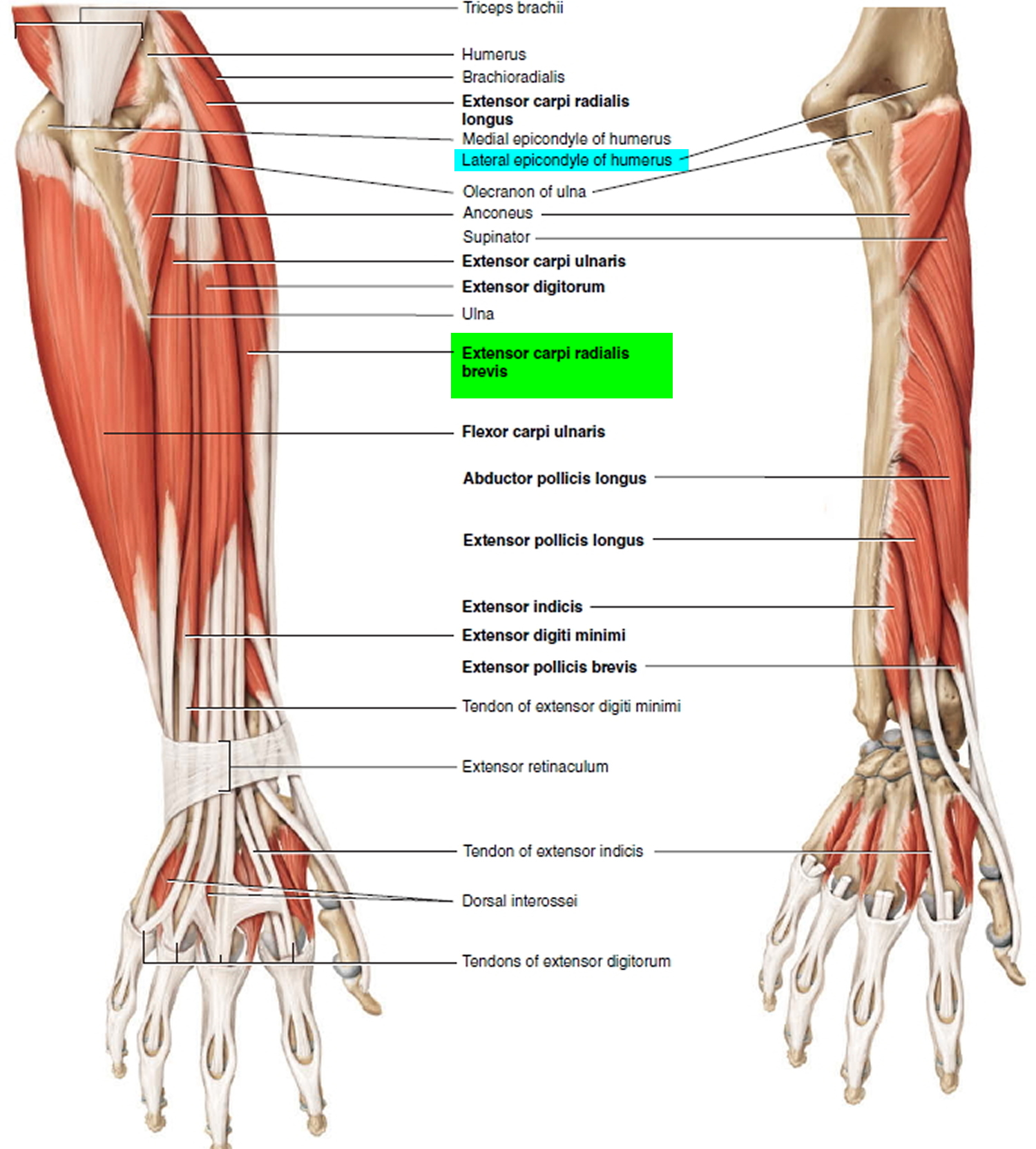
Tennis elbow is an inflammation of the tendons (usually the origin of the extensor carpi radialis brevis muscle) that join the forearm muscles on the outside of the elbow. The tendon usually involved in tennis elbow is called the Extensor Carpi Radialis Brevis. The extensor carpi radialis brevis muscle originates on the lateral epicondyle (thus the name lateral epicondylitis) of the humerus and inserts into metacarpal #3. Its function is extends and abducts the hand at the wrist joint. The forearm muscles and tendons become damaged from overuse — repeating the same motions again and again. This leads to pain and tenderness on the outside of the elbow.
There are many treatment options for tennis elbow. In most cases, treatment involves a team approach. Primary doctors, physical therapists, and, in some cases, surgeons work together to provide the most effective care.
Figure 3. Elbow joint
Causes of Elbow tendonitis
Overuse
Recent studies show that tennis elbow is often due to damage to a specific forearm muscle. The extensor carpi radialis brevis muscle helps stabilize the wrist when the elbow is straight. This occurs during a tennis groundstroke, for example. When the extensor carpi radialis brevis muscle is weakened from overuse, microscopic tears form in the tendon where it attaches to the lateral epicondyle. This leads to inflammation and pain.
The extensor carpi radialis brevis muscle may also be at increased risk for damage because of its position. As the elbow bends and straightens, the muscle rubs against bony bumps. This can cause gradual wear and tear of the muscle over time.
Activities
Athletes are not the only people who get tennis elbow. Many people with tennis elbow participate in work or recreational activities that require repetitive and vigorous use of the forearm muscle.
Painters, plumbers, and carpenters are particularly prone to developing tennis elbow. Studies have shown that auto workers, cooks, and even butchers get tennis elbow more often than the rest of the population. It is thought that the repetition and weight lifting required in these occupations leads to injury.
Age
Most people who get tennis elbow are between the ages of 30 and 50, although anyone can get tennis elbow if they have the risk factors. In racquet sports like tennis, improper stroke technique and improper equipment may be risk factors.
Unknown
Lateral epicondylitis can occur without any recognized repetitive injury. This occurence is called “insidious” or of an unknown cause.
Symptoms of Elbow tendonitis
The symptoms of tennis elbow develop gradually. In most cases, the pain begins as mild and slowly worsens over weeks and months. There is usually no specific injury associated with the start of symptoms.
Common signs and symptoms of tennis elbow include:
- Pain or burning on the outer part of your elbow
- Weak grip strength
The symptoms are often worsened with forearm activity, such as holding a racquet, turning a wrench, or shaking hands. Your dominant arm is most often affected; however both arms can be affected.
Diagnosis of Elbow tendonitis
Your doctor will consider many factors in making a diagnosis. These include how your symptoms developed, any occupational risk factors, and recreational sports participation.
Your doctor will talk to you about what activities cause symptoms and where on your arm the symptoms occur. Be sure to tell your doctor if you have ever injured
your elbow. If you have a history of rheumatoid arthritis or nerve disease, tell your doctor.
During the examination, your doctor will use a variety of tests to pinpoint the diagnosis. For example, your doctor may ask you to try to straighten your wrist and fingers against resistance with your arm fully straight to see if this causes pain. If the tests are positive, it tells your doctor that those muscles may not be healthy.
Tests:
- X-rays. These tests provide clear images of dense structures like bone. They may be taken to rule out arthritis of the elbow.
- Magnetic resonance imaging (MRI) scan. If your doctor thinks your symptoms are related to a neck problem, an MRI scan may be ordered. MRIs scans show details of soft tissues, and will help your doctor see if you have a possible herniated disk or arthritis in your neck. Both of these conditions often produce arm pain.
- Electromyography (EMG). Your doctor may order an EMG to rule out nerve compression. Many nerves travel around the elbow, and the symptoms of nerve compression are similar to those of tennis elbow.
Treatment of Elbow tendonitis
Nonsurgical Treatment
Approximately 80% to 95% of patients have success with nonsurgical treatment.
Rest. The first step toward recovery is to give your arm proper rest. This means that you will have to stop participation in sports or heavy work activities for several weeks.
Non-steroidal anti-inflammatory (NSAIDs) medicines. Drugs like aspirin or ibuprofen reduce pain and swelling.
Equipment check. If you participate in a racquet sport, your doctor may encourage you to have your equipment checked for proper fit. Stiffer racquets and looser-
strung racquets often can reduce the stress on the forearm, which means that the forearm muscles do not have to work as hard. If you use an oversized racquet,
changing to a smaller head may help prevent symptoms from recurring.
Physical therapy. Specific exercises are helpful for strengthening the muscles of the forearm. Your therapist may also perform ultrasound, ice massage, or muscle-stimulating techniques to improve muscle healing.
Brace. Using a brace centered over the back of your forearm may also help relieve symptoms of tennis elbow. This can reduce symptoms by resting the muscles and tendons.
Steroid injections. Steroids, such as cortisone, are very effective anti-inflammatory medicines. Your doctor may decide to inject your damaged muscle with a steroid to relieve your symptoms.
Extracorporeal shock wave therapy. Shock wave therapy sends sound waves to the elbow. These sound waves create “microtrauma” that promote the body’s natural healing processes. Shock wave therapy is considered experimental by many doctors, but some sources show it can be effective.
Platelet-rich plasma is currently being investigated for its effectiveness in speeding the healing of a variety of tendon injuries. Platelet-rich plasma is a preparation developed from a patient’s own blood. It contains a high concentration of proteins called growth factors that are very important in the healing of injuries. Current research on platelet-rich plasma and lateral epicondylitis is very promising. A few treatment centers across the country are incorporating platelet-rich plasma injections into the nonsurgical treatment regimen for lateral epicondylitis. However, this method is still under investigation and more research is necessary to fully prove platelet-rich plasma’s effectiveness.
Surgical Treatment
If your symptoms do not respond after 6 to 12 months of nonsurgical treatments, your doctor may recommend surgery.
Most surgical procedures for tennis elbow involve removing diseased muscle and reattaching healthy muscle back to bone.
The right surgical approach for you will depend on a range of factors. These include the scope of your injury, your general health, and your personal needs. Talk with your doctor about the options. Discuss the results your doctor has had, and any risks associated with each procedure.
Open surgery
The most common approach to tennis elbow repair is open surgery. This involves making an incision over the elbow.
Open surgery is usually performed as an outpatient surgery. It rarely requires an overnight stay at the hospital.
Arthroscopic surgery
Tennis elbow can also be repaired using miniature instruments and small incisions. Like open surgery, this is a same-day or outpatient procedure.
Surgical risks
As with any surgery, there are risks with tennis elbow surgery. The most common things to consider include:
- Infection
- Nerve and blood vessel damage
- Possible prolonged rehabilitation
- Loss of strength
- Loss of flexibility
- The need for further surgery
Rehabilitation
Following surgery, your arm may be immobilized temporarily with a splint. About 1 week later, the sutures and splint are removed.
After the splint is removed, exercises are started to stretch the elbow and restore flexibility. Light, gradual strengthening exercises are started about 2 months after surgery.
Your doctor will tell you when you can return to athletic activity. This is usually 4 to 6 months after surgery. Tennis elbow surgery is considered successful in 80% to 90% of patients. However, it is not uncommon to see a loss of strength.
Bicep tendonitis
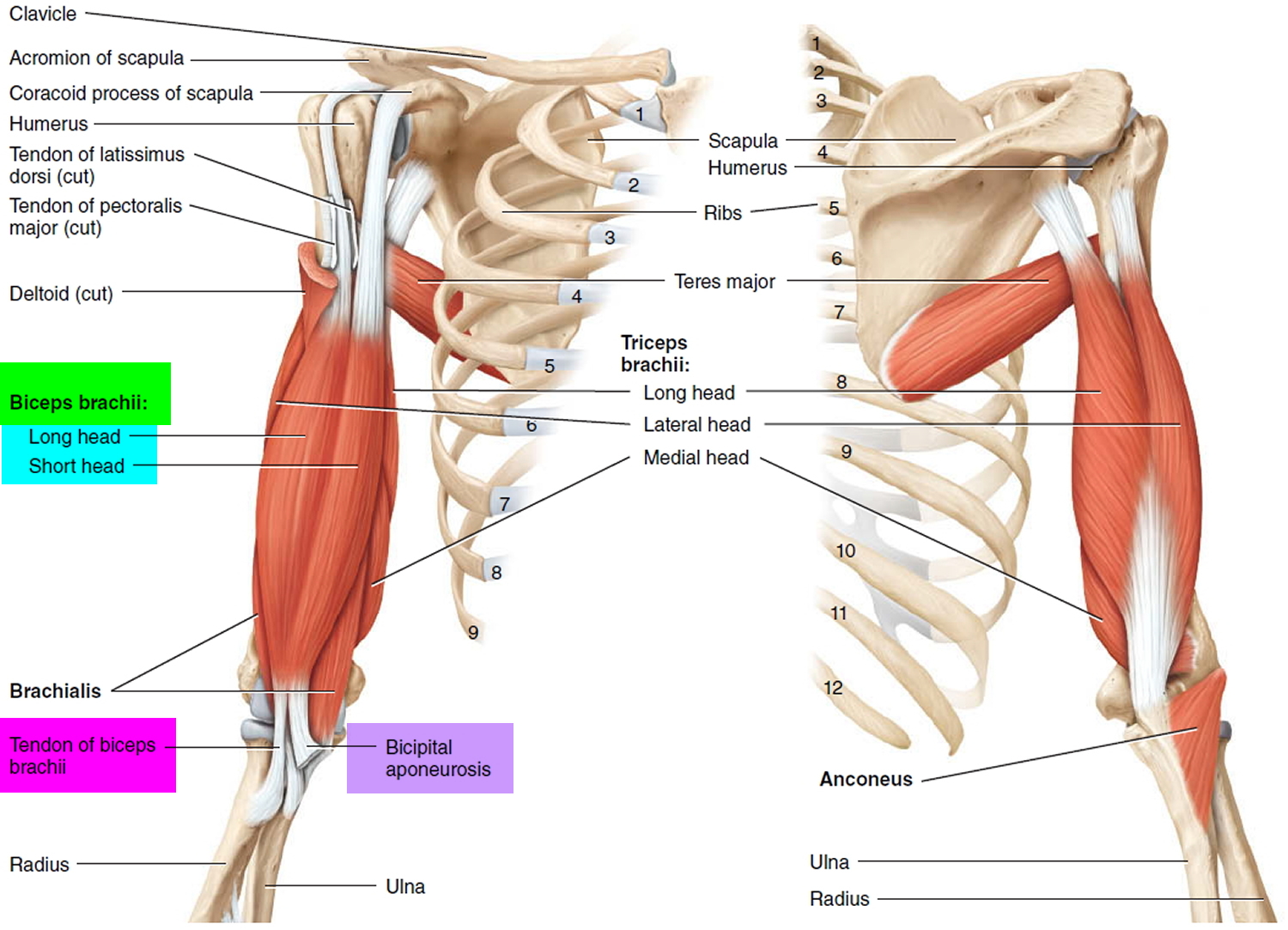
The biceps is the muscle in your upper arm that you flex when you bend your arm or show off your muscles. This muscle also helps you twist your forearm outward. Tough connective tissues called tendons attach the biceps muscle to the elbow and shoulder and help you move your arm.
The tendon that attaches the lower part of the biceps to the elbow is the distal tendon. The tendons that attach the top of the biceps muscle to the shoulder are the proximal tendons.
There are two proximal tendons — the long head and the short head. They attach to your shoulder blade in different places to hold the top of your upper arm bone firmly in your shoulder socket while still allowing it to move.
If any of these tendons become swollen or irritated from overuse, it can lead to a condition called biceps tendonitis. If you have biceps tendonitis, it can hurt just to move your arm. The good news is, most cases heal on their own with rest and medication.
Symptoms and signs of Proximal Biceps Tendonitis
Proximal biceps tendonitis usually starts out slowly and becomes more painful the more a person uses that arm. But sometimes an injury or small tear in the tendon can cause problems right away.
Some of the more common symptoms of proximal biceps tendonitis include 22:
- pain in the front or side of the shoulder and the upper arm
- pain in the arm at night, especially when you sleep on that side
- pain when you move your arm, raise it above your head, or reach behind you
- shoulder weakness and stiffness
- loss of some motion in the arm
Figure 4. Biceps muscles and tendons
What Causes Bicep tendonitis ?
The word “tendonitis” simply means that the tendon is irritated and swollen. In teens, biceps tendonitis is usually an overuse injury. Baseball pitchers, swimmers, tennis players, and people who have to reach above their heads a lot are at greater risk because of the repeated stress on their shoulders and upper arms.
Proximal biceps tendonitis often happens along with other shoulder problems. In most cases, there is also damage to another shoulder tendon called a rotator cuff tendon.
How Do Doctors Diagnose Bicep tendonitis ?
If your shoulder and upper arm hurt when you move your arm, and you’re worried that you might have biceps tendonitis, call a doctor.
The doctor will examine you and ask about any activities you’ve been doing that might have caused the problem. He or she will also check the strength and range of motion in your shoulder and look to see if it feels loose or unstable. For more serious cases (or to rule out other problems), the doctor might want you to have an X-ray, ultrasound, or magnetic resonance imaging (MRI) scan.
How Can you Prevent Biceps Tendonitis ?
The best way to prevent biceps tendonitis is to avoid activities that put your arms above your head a lot. But if you swim or play tennis or baseball, that might not be an option!
If your activities put you at risk for biceps tendonitis, you’ll want to do exercises that strengthen the muscles of your shoulder and upper arm. Strong muscles will keep the entire area more stable and less likely to get injured.
If you play a sport that puts you at greater risk of biceps tendonitis, make sure you know the right way to play. Playing in the wrong way can put your arm in weird positions that may put added stress on your shoulder. As much as you can, try to avoid reaching above your head or doing other things that require a lot of shoulder movement.
Most important, if you feel any pain in your shoulder or upper arm, stop doing the activity that might be causing it right away. Don’t start the activity again until the pain is gone or a doctor has told you it’s OK. Never try to ignore pain or play through it. This will most likely only make the condition worse.
Biceps Tendonitis Treatment
Most cases of biceps tendonitis can be treated at home with fairly simple methods. Although doctors sometimes need to do surgery to repair badly injured proximal biceps tendons, it’s usually for adults. Kids and teens almost never need surgery for this kind of injury.
Treatment can include the following:
- Rest your arm. Stop doing activities that require a lot of shoulder movement and try to avoid using your injured arm for any lifting or reaching.
- Ice the affected area. Apply ice or a cold compress to your shoulder for up to 20 minutes several times a day to help keep the swelling down. (Never apply ice directly to the skin.)
- Take anti-inflammatory medications. Painkillers such as ibuprofen can help relieve pain and reduce swelling in the shoulder and upper arm. The doctor also may recommend a cream or patch that can be applied to the skin. In some cases, doctors may give people steroid injections to ease pain and help reduce swelling.
- Do stretching and strengthening exercises. These will help strengthen your shoulder and restore its range of motion. Strengthening and stretching exercises can help you recover and make you less likely to reinjure your arm. A doctor or a physical therapist can work with you to develop a good exercise program.
The good news about proximal biceps tendonitis is that most cases heal just fine on their own. But it does require patience. The key with this kind of injury is to give your arm plenty of time to rest. You don’t want to jump back into your sport or activity too soon or you’ll risk making things worse and spending even more time on the sidelines.
Wrist Tendonitis
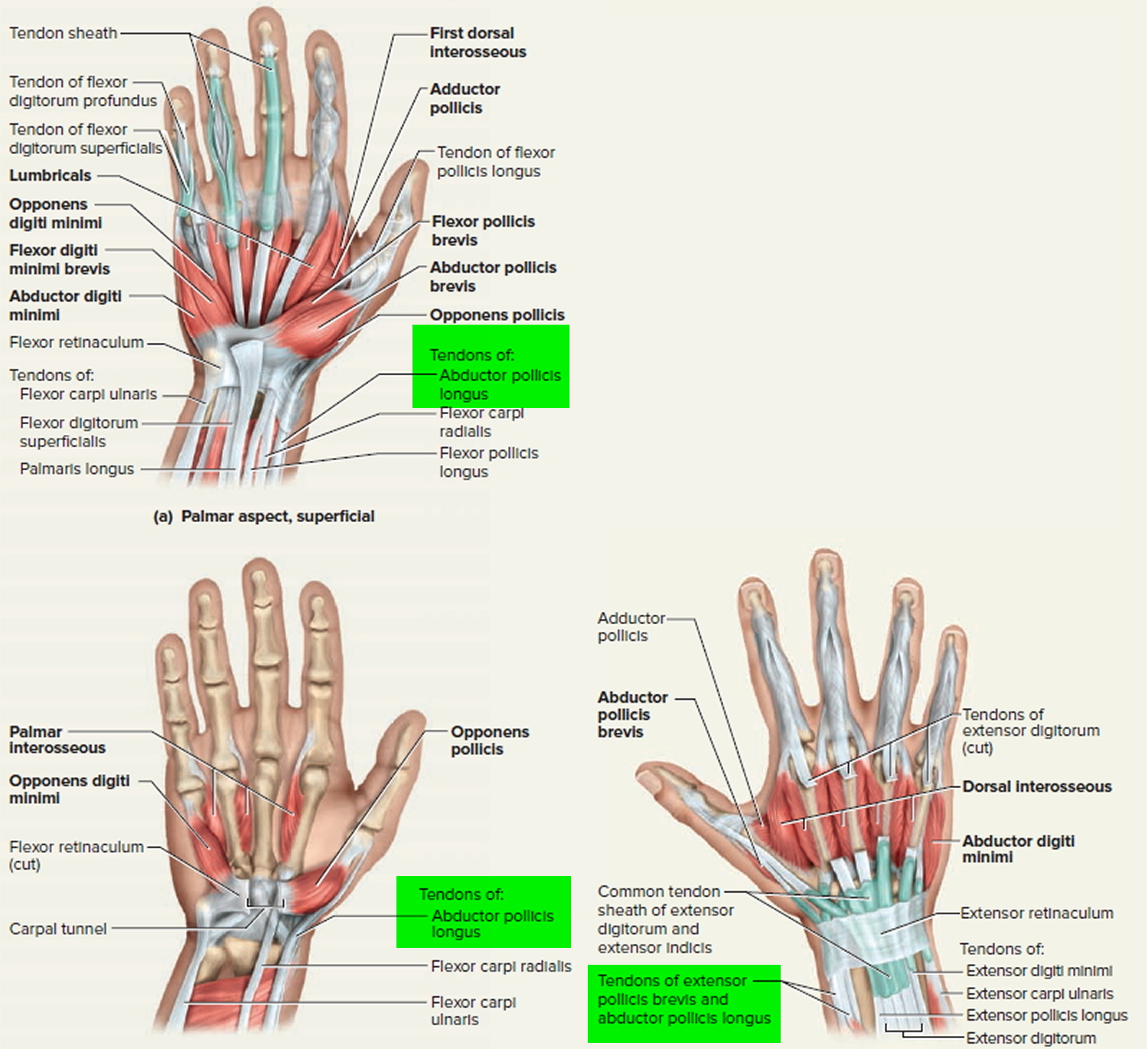
De Quervain’s tenosynovitis is a painful condition that affects the tendons in your wrist. It occurs when the 2 tendons around the base of your thumb become swollen 23. The swelling causes the sheaths (casings) covering the tendons to become inflamed. Swelling of the tendons, and the tendon sheath, can cause pain and tenderness along the thumb side of the wrist. This is particularly noticeable when forming a fi st, grasping or gripping something, or when turning the wrist. The swelling also puts pressure on nearby nerves, causing pain and numbness.
Two of the main tendons to the thumb pass through a tunnel (or series of pulleys) located on the thumb side of the wrist. Tendons are rope-like structures that attach muscle to bone. Tendons are covered by a slippery thin so -tissue layer, called synovium. This layer allows the tendons to slide easily through a fibrous tunnel called a sheath. Any swelling of the tendons and/or thickening of the sheath, results in increased friction and pain with certain thumb and wrist movements.
Figure 5. Wrist tendon (thumb tendons)
Symptoms of wrist tendonitis
The main symptom of de Quervain’s tenosynovitis is pain or tenderness at the base of your thumb. You might also feel pain going up your forearm. The pain may develop slowly or come on suddenly. It may get worse when you use your hand, thumb, or wrist.
Other symptoms include 24:
- Pain may be felt over the thumb side of the wrist. This is the main symptom. The pain may appear either gradually or suddenly. Pain is felt in the wrist and can travel up the forearm. The pain is usually worse when the hand and thumb are in use. This is especially true when forcefully grasping objects or twisting the wrist.
- Swelling near the base of your thumb. This swelling may accompany a fluid-filled cyst in this region.
- Pain and swelling may make it difficult to move the thumb and wrist.
- Numbness along the back of your thumb and index finger.
- A “catching” or “snapping” feeling when you move your thumb.
- A squeaking sound as the tendons move within the swollen sheaths.
What causes wrist tendonitis ?
The most common cause of de Quervain’s tenosynovitis is chronic overuse of the wrist. Repetitive movements day after day cause irritation and pain. One common movement that causes it is lifting a child into a car seat. Another is lifting heavy grocery bags by the handles. Other causes could include a direct injury to the wrist or inflammatory arthritis.
You are more likely to develop de Quervain’s tenosynovitis if:
- You are a woman.
- You are 40 years of age or older.
- Your hobby or job involves repetitive hand and wrist motions. This is a very common cause.
- You have injured your wrist. Scar tissue can restrict the movement of your tendons.
- You are pregnant. Hormonal changes during pregnancy can cause it.
- You have arthritis.
How is wrist tendonitis diagnosed ?
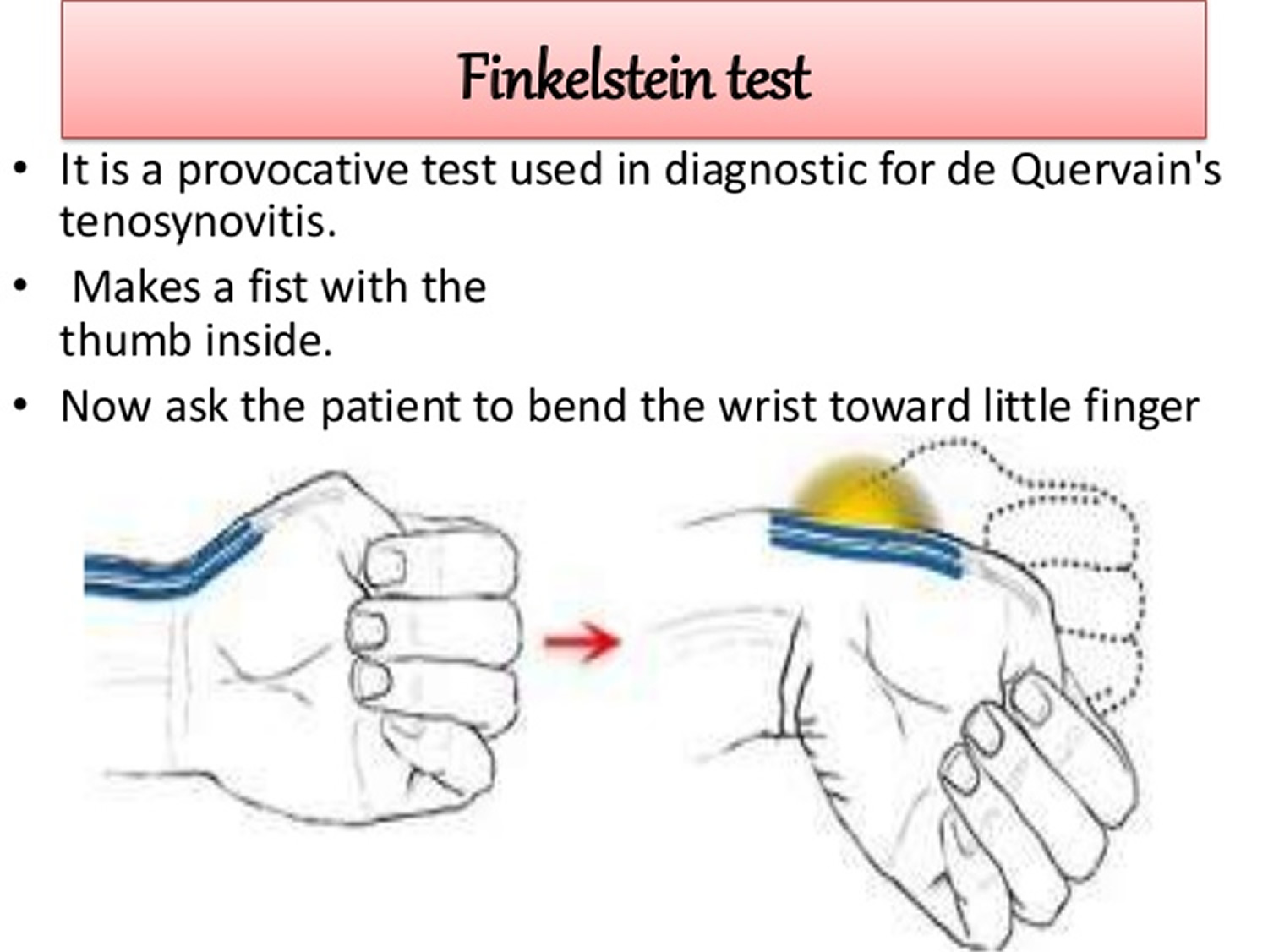
To diagnose de Quervain’s tenosynovitis, your doctor may do a simple test. It is called the Finkelstein test. First, you bend your thumb so it rests across your palm. Then you make a fist, closing your fingers over your thumb. Last, you bend your wrist toward your little finger. If you have tenderness or pain at the base of your thumb, you probably have de Quervain’s tenosynovitis.
Figure 6. Finkelstein test
Other tests such as X-rays usually aren’t needed to diagnose the condition.
Can wrist tendonitis be prevented or avoided ?
The best way to prevent de Quervain’s tenosynovitis is to avoiding repetitive movements. Change your actions to reduce the stress on your wrists. Take frequent breaks to rest if you are using your wrists. Wear a brace or splint on your thumb and wrist, if necessary.
Follow the exercise routine suggested by your doctor or physical therapist. Be sure to tell him or her about any activities that cause pain, numbness, or swelling.
Treatment for wrist tendonitis
Treatment for de Quervain’s tenosynovitis focuses on reducing pain and swelling. It includes:
- Applying heat or ice to the affected area.
- Taking a nonsteroidal anti-inflammatory drug (NSAID). These include ibuprofen (Advil, Motrin) or naproxen (Aleve).
- Avoiding activities that cause pain and swelling. Especially avoid those that involve repetitive hand and wrist motions.
- Wearing a splint 24 hours a day for 4 to 6 weeks to rest your thumb and wrist.
- Getting injections of corticosteroids or a local anesthetic (numbing medicine) into the tendon sheath. These injections are very effective and are used regularly.
A physical therapist or occupational therapist can show you how to change the way you move. This can reduce stress on your wrist. He or she can also teach you exercises to strengthen your muscles.
Most people notice improvement after 4 to 6 weeks of treatment. They are able to use their hands and wrists without pain once the swelling is gone.
You might need surgery if your case is severe or if other treatments don’t relieve your pain.
Surgical Treatment
Surgery may be recommended if symptoms are severe or do not improve. The goal of surgery is to open the thumb compartment (covering) to make more room for the irritated tendons.
Regardless of the treatment, normal use of the hand usually can be resumed once comfort and strength have returned. Your orthopaedic surgeon can advise you on the best treatment for your situation.
Patellar tendonitis
Jumper’s knee — also known as patellar tendonitis or patellar tendinopathy — is an inflammation or injury of the patellar tendon, the cord-like tissue that joins the patella (kneecap) to the tibia (shin bone). Jumper’s knee is an overuse injury (when repeated movements cause tissue damage or irritation to a particular area of the body) 25.
Constant jumping, landing, and changing direction can cause strains, tears, and damage to the patellar tendon. So kids who regularly play sports that involve a lot of repetitive jumping — like track and field (particularly high-jumping), basketball, volleyball, gymnastics, running, and soccer — can put a lot of strain on their knees.
Jumper’s knee can seem like a minor injury that isn’t really that serious. Because of this, many athletes keep training and competing and tend to ignore the injury or attempt to treat it themselves. But it’s important to know that jumper’s knee is a serious condition that can get worse over time and ultimately require surgery. Early medical attention and treatment can help prevent continued damage to the knee.
How the Knee Works
To understand how jumper’s knee happens, it helps to understand how the knee works. The knee, which is the largest joint in the body, provides stability to the leg and allows it to bend, swivel, and straighten. Several parts of the body interact to allow the knee to function properly:
Bones like the femur (thighbone), the tibia (shinbone), and the patella (kneecap) give the knee the strength needed to support the weight of the body. The bones that meet at the knee allow it to bend smoothly.
Muscles provide the tug on the bones needed to bend, straighten, and support joints. The muscles around the knee include the quadriceps (at the front of the thigh) and the hamstring (on the back of the thigh). The quadriceps muscle helps straighten and extend the leg, and the hamstring helps bend the knee.
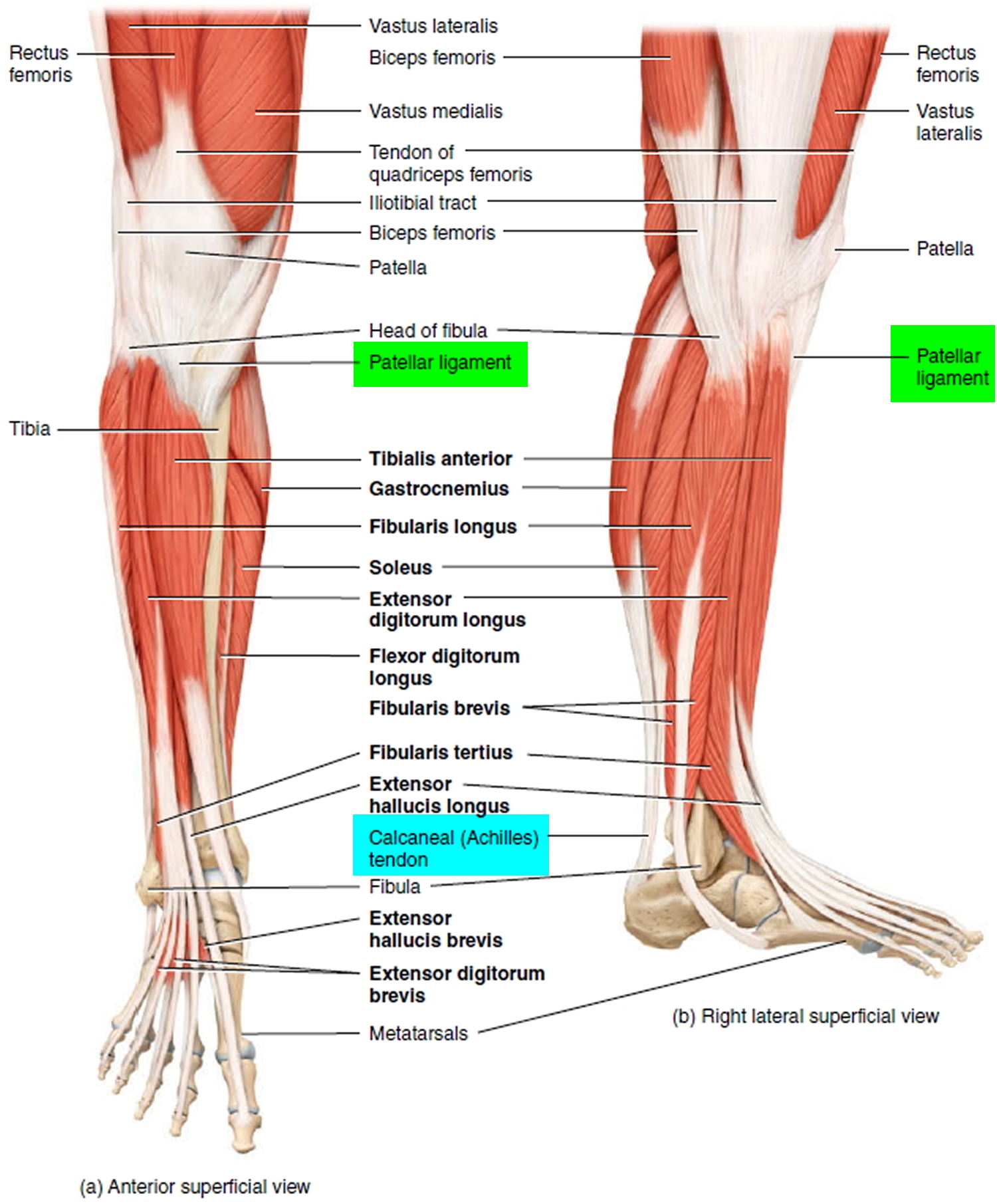
Tendons are strong bands of tissue that connect muscles to bones. The tendons in the front of the knee are the quadriceps tendon and the patellar tendon. The quadriceps tendon connects to the top of the patella and allows the leg to extend. The patellar tendon connects to the bottom of the kneecap and attaches to the top of the tibia.
Similar to tendons, ligaments are strong bands of tissue that connect bones to other bones.
By working together, bones, muscles, tendons, and ligaments enable the knee to move, bend, straighten, provide strength to jump, and stabilize the leg for landing.
When the knee is extended, the quadriceps muscle pulls on the quadriceps tendon, which in turn pulls on the patella. Then, the patella pulls on the patellar tendon and the tibia and allows the knee to straighten. In contrast, when bending the knee, the hamstring muscle pulls on the tibia, which causes the knee to flex.
In jumper’s knee, the patellar tendon is damaged. Since this tendon is crucial to straightening the knee, damage to it causes the patella to lose any support or anchoring. This causes pain and weakness in the knee, and leads to difficulty in straightening the leg.
Figure 7. Ligaments and tendons of the knee
Symptoms of Patellar tendonitis
Common symptoms of jumper’s knee include:
- pain directly over the patellar tendon (or more specifically, below the kneecap)
- stiffness of the knee, particularly while jumping, kneeling, squatting, sitting, or climbing stairs
- pain when bending the knee
- pain in the quadriceps muscle
- leg or calf weakness
Less common symptoms include:
- balance problems
- warmth, tenderness, or swelling around the lower knee
Treatment of Patellar tendonitis
Jumper’s knee is first evaluated by a grading system that measures the extent of the injury (grades range from 1 to 5, with grade 1 being pain only after intense activity and grade 5 being daily constant pain and the inability to participate in any sporting activities).
While examining the knee, a doctor or medical professional will ask the person to run, jump, kneel, or squat to determine the level of pain. In addition, an X-ray or MRI might be recommended. Depending on the grade of the injury, treatment can range from rest and icepacks to surgery.
For mild to moderate jumper’s knee, treatment includes:
- resting from activity or adapting a training regimen that greatly reduces any jumping or impact
- icing the knee to reduce pain and inflammation
- wearing a knee support or strap (called an intrapatellar strap or a Chopat strap) to help support the knee and patella. The strap is worn over the patellar tendon, just beneath the kneecap. A knee support or strap can help minimize pain and relieve strain on the patellar tendon.
- elevating the knee when it hurts (for example, placing a pillow under the leg)
- anti-inflammatory medications, like ibuprofen, to minimize pain and swelling
- massage therapy
- minimum-impact exercises to help strengthen the knee
- rehabilitation programs that include muscle strengthening, concentrating on weight-bearing muscle groups like the quadriceps and calf muscles
- specialized injections to desensitize nerve endings and reduce inflammation
On rare occasions, such as when there’s persistent pain or the patellar tendon is seriously damaged, jumper’s knee requires surgery. Surgery includes removing the damaged portion of the patellar tendon, removing inflammatory tissue from the lower area (or bottom pole) of the patella, or making small cuts on the sides of the patellar tendon to relieve pressure from the middle area.
After surgery, a rehabilitation program involving strengthening exercises and massage is followed for several months to a year.
Recovery
Recovering from jumper’s knee can take a few weeks to several months. It’s best to stay away from any sport or activity that can aggravate the knee and make conditions worse.
But, recovering from jumper’s knee doesn’t mean that someone can’t participate in any sports or activities. Depending on the extent of the injury, low-impact sports or activities can be substituted (for instance, substituting swimming for running). Your doctor will let you know what sports and activities are off-limits during the healing process.
Preventing Jumper’s Knee
The most important factor in preventing jumper’s knee is stretching. A good warm-up regimen that involves stretching the quadriceps, hamstring, and calf muscles can help prevent jumper’s knee. It’s always a good idea to stretch after exercising, too.
Peroneal tendonitis
The peroneal (fibularis muscles) tendons run on the outside of the ankle just behind the bone called the fibula. Tendons connect muscle to bone and allow them to exert their force across the joints that separate bones. Ligaments, on the other hand, connect bone to bone. Tendinitis implies that there is inflammation, enlargement and thickening with swelling of the tendon. This usually occurs in the setting of overuse, meaning a patient or athlete does a repetitive activity that irritates the tendon over long periods of time. However, in studies that have taken the tendons and looked at them under a microscope, there really are not the types of inflammatory cells once thought. There is really more of an enlargement and thickening of the tendon. This is better termed tendinosis.
People with peroneal tendinitis typically have either tried a new exercise or have markedly increased their activities. Characteristic activities include marathon running or others which require repetitive use of the ankle. Patients will usually present with pain right around the back of the ankle. There is usually no history of a specific injury.
What causes peroneal tendinitis ?
As discussed above, improper training or rapid increases in training and poor shoewear can lead to peroneal tendinitis. Also, patients who have a hindfoot varus (turning inward) posture may be more susceptible. This is because in those patients, the heel is slightly turned inwards which requires that the peroneal tendons work harder. Their main job is to evert or turn the ankle to the outside, which fights against the varus position. The harder the tendons work, the more likely they are to develop tendinitis.
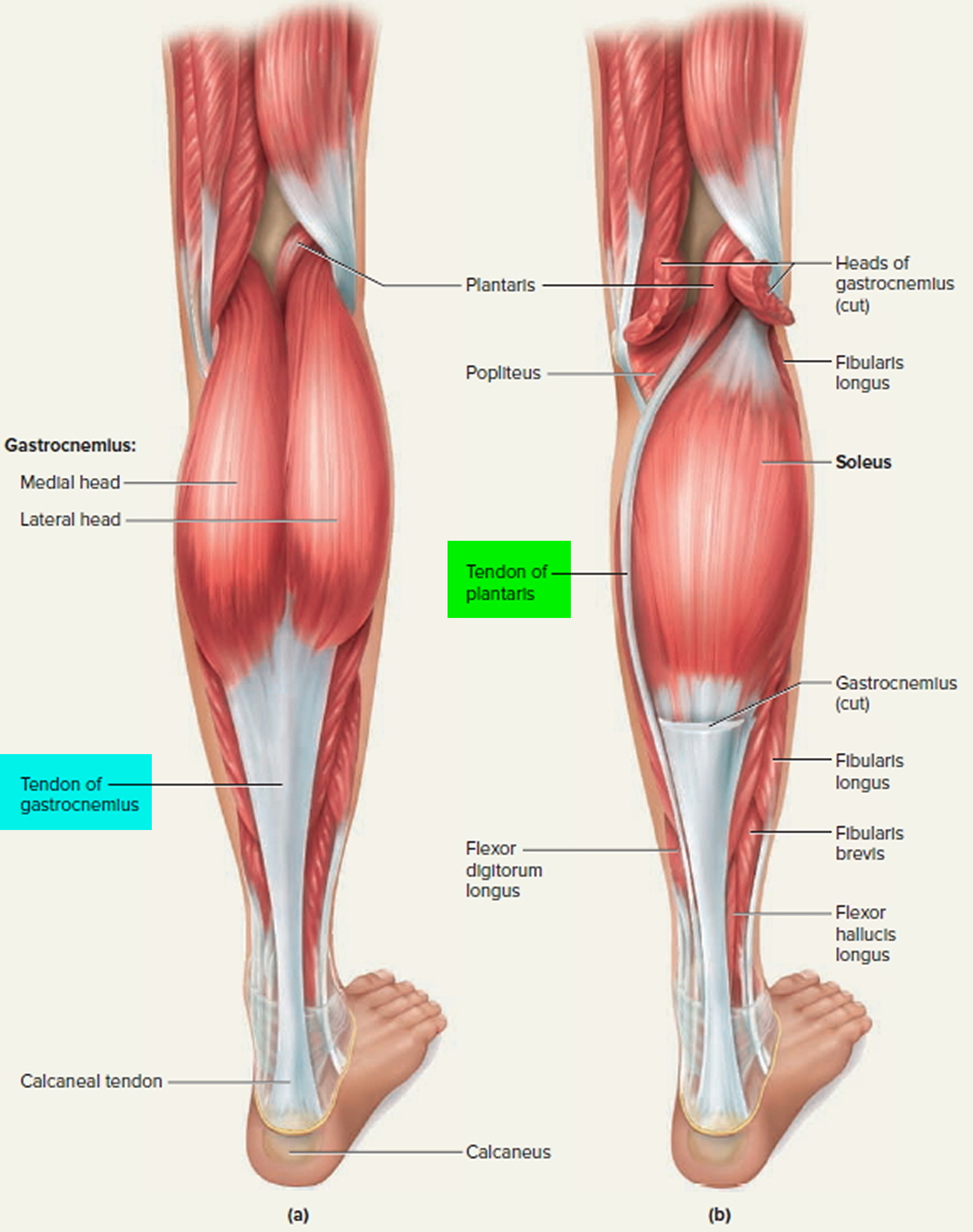
Figure 8. Tendons of the calf and foot (back of leg)
How is peroneal tendonitis diagnosed ?
The diagnosis of peroneal tendonitis can be made in large part by history (i.e. the story a patient tells). As noted above, patients will have an overuse activity, rapid increase in recent activity, or other training errors and will have pain in the back and outside of the ankle. There is pain on exam to palpation right on the peroneal tendons. I t is important to distinguish this from pain over the fibula, which might indicate a different problem (i.e. stress reaction of the bone). Pain on the fibula occurs directly over the bone which is easily palpated. Pain in the peroneals occurs slightly further behind. There is also pain with inversion or carrying the ankle to the outside. Patients may also have weakness in trying to bring the ankle to the outside (i.e. in eversion). It is important to look for the varus posturing of the heel which, as noted above, means that the heel is turned inwards. This can predispose a patient to the problem. The workup can also include using radiology. X-rays will typically be normal. Ultrasound is a very effective and relatively inexpensive way to assess the tendons and can show an abnormal appearance or tear which sometimes occurs. An MRI is also equally important and can also show a tear.
What are treatment options for peroneal tendonitis ?
The vast majority of peroneal tendinosis will heal without surgery. This is because it is an overuse injury and can heal with rest. If there is significant pain, a CAM Walker boot for several weeks is a good idea. If there really is no tenderness with walking, an ankle brace might be the next best step. Patients should very much limit how much they are walking or on their feet until the pain abates. This usually takes several weeks. Resumption of training can then occur, but must occur very slowly and be based on pain. For those patients who have hindfoot varus, as noted above, an orthotic that tilts the ankle to the opposite side may well help to offload the tendons. It is important to talk to your doctor about changing your training. This includes using new shoes for running or also cross-training, which means alternating activities each day. Physical therapy is also very important. This, as with ankle sprains, can be done to strengthen the tendons.
There is some interest at the moment in using platelet-rich plasma to help stimulate healing growth. Currently, there are no studies showing that this works for the peroneal tendons. Steroids are probably best avoided as they can actually damage tendon. Surgical treatment is indicated if the pain does not get better with rest. Conservative treatment – that is, without surgery – should last, however, even up to a year before considering surgery. If there is a tear, meaning a split that runs along the length of the tendons, one could consider cleaning it out and repairing the tendon. Sometimes, making the groove in the back of the bone of the fibula deeper allows the tendons more space and can help as well. Finally, if the tendon is very bad, one may need to resect the tendon and connect both the longus and brevis together. Only the specific tendon involved should be addressed. Occasionally, both may be involved.
How long is the recovery for peroneal tendonitis ?
Patients usually recover fully but this can take considerable time. You must be patient and allow the tendon to heal before going back to activity. If you need surgery, your recovery time may be substantial. You may be instructed not to put your foot down with weight for about six weeks. Your orthopaedic foot and ankle surgeon likely will order physical therapy ensue.
The outcome is usually good. However, sometimes it takes time for people to get back to their activity. When a tear develops and there is chronic thickening of the tendon, the outcomes are not as good.
Potential Complications of peroneal tendonitis
If the tendinosis is not addressed, tearing of the tendon can occur. Also, weakness of the tendons can lead to an ankle sprain. In the case of surgery, infection can develop. Nerve damage can occur if the sural nerve which runs along the side of the foot and provides sensation to the foot is cut or stretched. Instability itself can lead to many sprains which can damage the cartilage on the inside of the ankle.
Posterior tibial tendonitis
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot.
Posterior tibial tendon dysfunction is often called adult acquired flatfoot because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. Posterior tibial tendon dysfunctionis usually progressive, which means it will keep getting worse, especially if it is not treated early.
Causes of Posterior tibial tendonitis
Overuse of the posterior tibial tendon is often the cause of posterior tibial tendon dysfunction. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking or climbing stairs.
Symptoms of Posterior tibial tendonitis
The symptoms of posterior tibial tendon dysfunction may include pain, swelling, a flattening of the arch and an inward rolling of the ankle. As the condition progresses, the symptoms will change.
For example, when posterior tibial tendon dysfunctioninitially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm and swollen.
Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward.
As posterior tibial tendon dysfunction becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably, and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Nonsurgical Treatment of Posterior tibial tendonitis
Because of the progressive nature of posterior tibial tendon dysfunction, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery, and progression of your condition can be arrested.
In contrast, untreated posterior tibial tendon dysfunction could leave you with an extremely flat foot, painful arthritis in the foot and ankle and increasing limitations on walking, running or other activities.
In many cases of posterior tibial tendon dysfunction, treatment can begin with nonsurgical approaches that may include:
- Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe.
- Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weightbearing for a while.
- Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization.
- Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation.
- Shoe modifications. Your foot and ankle surgeon may advise changes to your shoes and may provide special inserts designed to improve arch support.
When Is Surgery Needed ?
In cases of posterior tibial tendon dysfunction that have progressed substantially or have failed to improve with nonsurgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Foot Tendonitis
Achilles (calcaneal) tendinitis occurs when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It allows you to push your foot down. You use your Achilles tendon when walking, running, and jumping.
Achilles tendinitis is a common condition that causes pain along the back of the leg near the heel.
Types of foot (Achilles) tendinitis
Noninsertional Achilles Tendinitis
- In noninsertional Achilles tendinitis, fibers in the middle portion of the tendon have begun to break down with tiny tears (degenerate), swell, and thicken.
- Tendinitis of the middle portion of the tendon more commonly affects younger, active people.
Insertional Achilles Tendinitis
- Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches (inserts) to the heel bone.
In both noninsertional and insertional Achilles tendinitis, damaged tendon fibers may also calcify (harden). Bone spurs (extra bone growth) often form with insertional Achilles tendinitis.
Tendinitis that affects the insertion of the tendon can occur at any time, even in patients who are not active.
Causes of foot tendonitis
There are two large muscles in the calf. These create the power needed to push off with the foot or go up on the toes. The large Achilles tendon connects these muscles to the heel.
Heel pain is most often due to overuse of the foot – from repetitive stress to the tendon. Rarely, it is caused by an injury.
Tendinitis due to overuse is most common in younger people. It can occur in walkers, runners, or other athletes.
This often happens when you push your bodies to do too much, too soon, but other factors can make it more likely to develop tendinitis, including 26:
- There is a sudden increase in the amount or intensity of an activity.
- Your calf muscles are very tight (not stretched out). Having tight calf muscles and suddenly starting an aggressive exercise program can put extra stress on the Achilles tendon.
- Bone spur—Extra bone growth where the Achilles tendon attaches to the heel bone can rub against the tendon and cause pain.
- You run on hard surfaces, such as concrete.
- You run too often.
- You jump a lot (such as when playing basketball).
- You DO NOT wear shoes that give your feet proper support.
- Your foot suddenly turns in or out.
Tendinitis from arthritis is more common in middle-aged and older adults. A bone spur or growth may form in the back of the heel bone. This may irritate the Achilles tendon and cause pain and swelling. Flat feet will put more tension on the tendon.
Prevention foot tendonitis
Exercises to keep your calf muscles strong and flexible will help reduce the risk of tendinitis. Overusing a weak or tight Achilles tendon makes you more likely to develop tendinitis.
Symptoms of foot tendonitis
Common symptoms of Achilles tendinitis include:
- Pain in the heel and along the length of the calcaneal (Achilles) tendon when walking or running.
- Pain and stiffness along the Achilles tendon in the morning.
- Severe pain the day afer exercising.
- The tendon may be painful to touch or move.
- Thickening of the tendon.
- The area may be swollen and warm.
- You may have trouble standing up on one toe.
- Swelling that is present all the time and gets worse throughout the day with activity.
Achilles tendinitis diagnosis
The health care provider will perform a physical exam. They will look for tenderness along the tendon and pain in the area of the tendon when you stand on your toes.
X-rays can help diagnose bone problems.
An MRI of the foot scan may be done if you are considering surgery or there is a chance that you have a tear in the Achilles tendon.
Treatment of foot tendonitis
The main treatments for Achilles tendinitis DO NOT involve surgery 27. It is important to remember that it may take at least 2 to 3 months for the pain to go away.
Try putting ice on the Achilles tendon area for 15 to 20 minutes, 2 to 3 times per day. Remove the ice if the area gets numb.
Changes in activity may help manage the symptoms:
- Decrease or stop any activity that causes pain.
- Run or walk on smoother and softer surfaces.
- Switch to biking, swimming, or other activities that put less stress on the Achilles tendon.
Your provider or physical therapist can show you stretching exercises for the Achilles tendon.
You may also need to make changes in your footwear, such as:
- Using a brace, boot or cast to keep the heel and tendon still and allow the swelling to go down
- Placing heel lifts in the shoe under the heel
- Wearing shoes that are softer in the areas over and under the heel cushion
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen, can help ease pain or swelling.
If these treatments DO NOT improve symptoms, you may need surgery to remove inflamed tissue and abnormal areas of the tendon. If there is a bone spur irritating the tendon, surgery can be used to remove the spur.
Extracorporeal shock wave therapy may be an alternative to surgery for people who have not responded to other treatments 28. This treatment uses low-dose sound waves. Extracorporeal shock wave therapy has not shown consistent results and therefore, is not commonly performed. However, because of the minimal risk involved, extracorporeal shock wave therapy is sometimes tried before surgery is considered.
Exercise
The following exercise can help to strengthen the calf muscles and reduce stress on the Achilles tendon.
- Calf stretch: Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch.
- Eccentric Strengthening Protocol 29. Eccentric strengthening is defined as contracting (tightening) a muscle while it is getting longer. Eccentric strengthening exercises can cause damage to the Achilles tendon if they are not done correctly. At first, they should be performed under the supervision of a physical therapist. Once mastered with a therapist, the exercises can then be done at home. These exercises may cause some discomfort, however, it should not be unbearable.
- Frequency: Three sets of 15 exercises, twice daily (total of 90 repetitions).
- Progression: Use same weight for first 1 to 2 weeks to achieve relative comfort with recommended daily frequency, then add weight (e.g., loaded backpacks, weighted vests) as comfort allows.
- Duration: Typical regimens last 12 weeks. Goal is a return to pain-free function with provocative activities, such as running.
Figure 9. Eccentric exercises for Achilles tendinitis
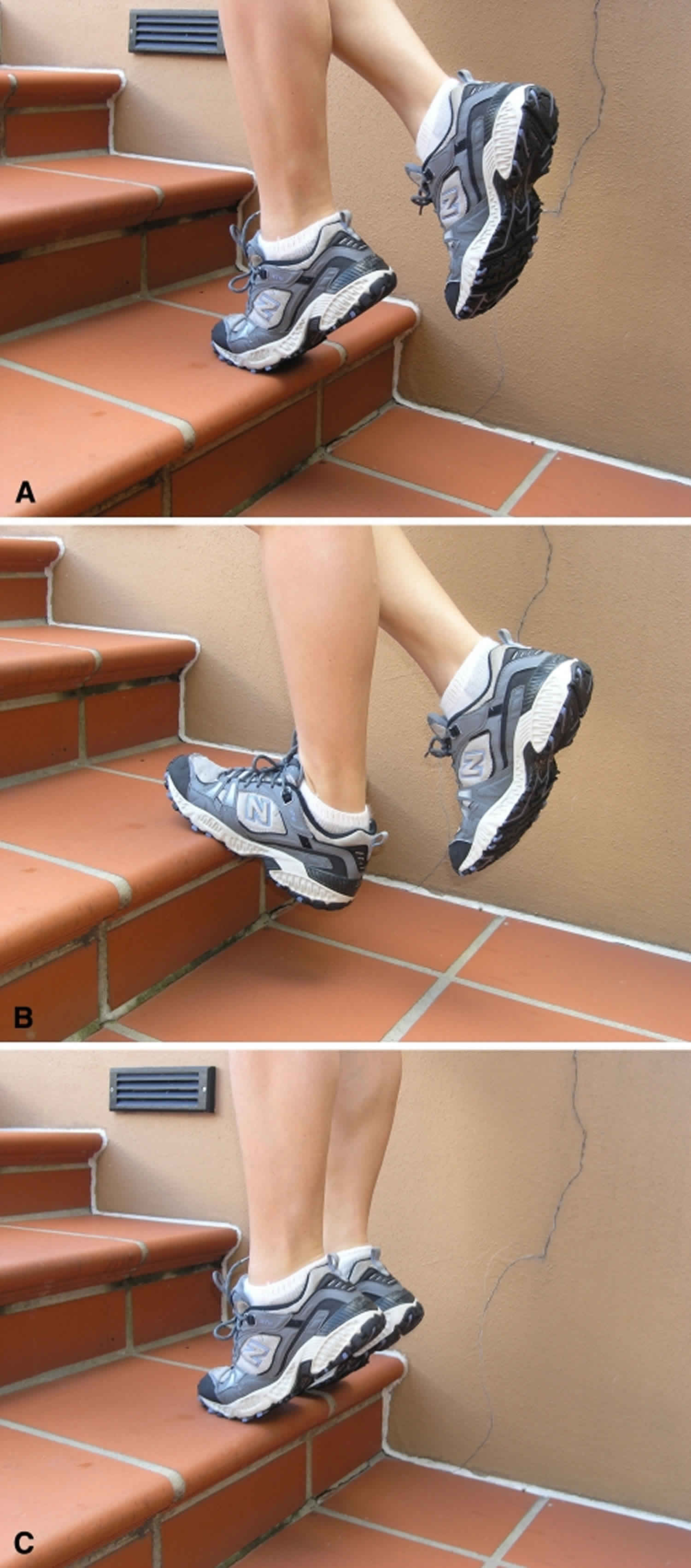
Footnote: An eccentric training protocol for the treatment of Achilles tendinopathy is demonstrated. (A) The patient starts in a single-leg standing position with the weight on the forefoot and the ankle in full plantar flexion. (B) The Achilles is then eccentrically loaded by slowly lowering the heel to a dorsiflexed position. (C) The patient then returns to the starting position using the arms or contralateral leg for assistance to avoid concentric loading of the involved Achilles tendon.
[Source 1]Supportive shoes and orthotics
Pain from insertional Achilles tendinitis is often helped by certain shoes, as well as orthotic devices. For example, shoes that are softer at the back of the heel can reduce irritation of the tendon. In addition, heel lifts can take some strain off the tendon.
Heel lifts are also very helpful for patients with insertional tendinitis because they can move the heel away from the back of the shoe, where rubbing can occur. They also take some strain off the tendon. Like a heel lift, a silicone Achilles sleeve can reduce irritation from the back of a shoe.
If your pain is severe, your doctor may recommend a walking boot for a short time. This gives the tendon a chance to rest before any therapy is begun. Extended use of a boot is discouraged, though, because it can weaken your calf muscle.
Surgical Treatment
Surgery should be considered to relieve Achilles tendinitis only if the pain does not improve after 6 months of nonsurgical treatment. The specific type of surgery
depends on the location of the tendinitis and the amount of damage to the tendon.
Gastrocnemius recession
This is a surgical lengthening of the calf (gastrocnemius) muscles. Because tight calf muscles place increased stress on the Achilles tendon, this procedure is useful for patients who still have difficulty flexing their feet, despite consistent stretching.
In gastrocnemius recession, one of the two muscles that make up the calf is lengthened to increase the motion of the ankle. The procedure can be performed with a traditional, open incision or with a smaller incision and an endoscope—an instrument that contains a small camera. Your doctor will discuss the procedure that best meets your needs. Complication rates for gastrocnemius recession are low, but can include nerve damage.
Gastrocnemius recession can be performed with or without débridement, which is removal of damaged tissue.
Debridement and repair (tendon has less than 50% damage)
The goal of this operation is to remove the damaged part of the Achilles tendon. Once the unhealthy portion of the tendon has been removed, the remaining tendon is repaired with sutures, or stitches to complete the repair.
In insertional tendinitis, the bone spur is also removed. Repair of the tendon in these instances may require the use of metal or plastic anchors to help hold the Achilles tendon to the heel bone, where it attaches. After débridement and repair, most patients are allowed to walk in a removable boot or cast within 2 weeks, although this period depends upon the amount of damage to the tendon.
Debridement with tendon transfer (tendon has greater than 50% damage)
In cases where more than 50% of the Achilles tendon is not healthy and requires removal, the remaining portion of the tendon is not strong enough to function alone. To prevent the remaining tendon from rupturing with activity, an Achilles tendon transfer is performed. The tendon that helps the big toe point down is moved to the heel bone to add strength to the damaged tendon. Although this sounds severe, the big toe will still be able to move, and most patients will not notice a change in the way they walk or run.
Depending on the extent of damage to the tendon, some patients may not be able to return to competitive sports or running.
Recovery after surgery
Most patients have good results from surgery. The main factor in surgical recovery is the amount of damage to the tendon. The greater the amount of tendon involved, the longer the recovery period, and the less likely a patient will be able to return to sports activity.
Physical therapy is an important part of recovery. Many patients require 12 months of rehabilitation before they are pain-free.
Complications after surgery
Moderate to severe pain after surgery is noted in 20% to 30% of patients and is the most common complication. In addition, a wound infection can occur and the infection is very difficult to treat in this location.
Outlook (Prognosis) for foot tendonitis
In most cases, lifestyle changes help improve symptoms. Keep in mind that symptoms may return if you DO NOT limit activities that cause pain, or if you DO NOT maintain the strength and flexibility of the tendon.
Possible Complications of foot tendonitis
Achilles tendinitis may make you more likely to have an Achilles rupture. This condition most often causes a sharp pain that feels as if you have been hit in the back of the heel with a stick. Surgical repair is necessary. However, the surgery may not be as successful as usual because there is already damage to the tendon.
Proximal hamstring tendinopathy
Proximal hamstring tendinopathy is commonly seen in runners of all distances 30. Anatomically, the semitendinosus and the long head of the biceps femoris muscles combine to create a conjoined tendon that inserts medially on the ischial tuberosity and sacrotuberous ligament, abutted by the insertion of the semimembranosus more laterally on the tuberosity 31. The inferior border of the gluteus maximus and the sciatic nerve are within close proximity to the tendon 31. It is presumed that overuse, poor lumbopelvic stability, and relatively weak hamstring musculature contribute to the development of proximal hamstring tendinopathy 32.
Runners with proximal hamstring tendinopathy often present with pain located near the ischial tuberosity of the affected limb that can extend down the posterior thigh.7,10,15,22 Sciatic nerve involvement and related symptoms, as evidenced by surgical exploratory findings, are often reported due to the sciatic nerve’s proximity to the site of injury 32. The sciatic nerve may be directly irritated by the proximal hamstring injury, creating true sciatic nerve involvement; however, most often proximal hamstring tendinopathy mimics sciatica by causing hamstring pain that refers down the posterior thigh. Common symptoms include pain with prolonged sitting, primarily on hard surfaces; pain with forward flexion of the trunk; and pain with running, often noted in the later part of the swing phase. Several diagnostic physical exam maneuvers have been described, including the Puranen-Orava test, the bent-knee stretch test, the modified bent-knee stretch test 33 and the supine 1-legged bridge 32. Table 1 lists common symptoms and physical exam findings seen in individuals with proximal hamstring tendinopathy.
Figure 10. Puranen-Orava test

Table 1. Common symptoms and physical examination findings with proximal hamstring tendinopathy
| Symptoms | Physical Exam Findings |
|---|---|
| Pain with trunk forward bending (passive hip flexion and knee extension) | Tenderness around the area of the ischial tuberosity |
| Localized pain in the area of the ischial tuberosity with prolonged sitting | Positive Puranen-Orava test |
| Referred pain down the posterior thigh, sometimes past the knee | Positive bent-knee stretch test |
| Pain with active hip extension and often knee flexion | Positive modified bent-knee stretch test |
| Pain worse with running | Positive supine 1-legged bridge (supine plank) test Excessive anterior pelvic tilt Possibly a positive seated slump test |
Magnetic resonance imaging and ultrasound have both been used to aid in diagnosis, with magnetic resonance imaging providing higher sensitivity 34. Common imaging features include increased tendon size, peritendinous T2 signal with a distal feathery appearance, and ischial tuberosity edema 35
The majority of the existing literature on the treatment of proximal hamstring tendinopathy revolves around surgical intervention, which has traditionally been reserved to address complete acute tears; however, recently, surgery has also been used to repair partial tears 36. Several nonsurgical options have been described for the treatment of proximal hamstring tendinopathy, including shockwave therapy 37, eccentric exercises with trunk/pelvis musculature strengthening 38, corticosteroid injection 39, massage/soft tissue mobilization, platelet-rich plasma injection 40 and a combined chiropractic approach 41. A recent description of 2 runners with proximal hamstring tendinopathy reported positive results with conservative treatment consisting of eccentric strengthening, lumbopelvic stabilization exercises, and trigger point dry needling of the hamstring and adductor magnus muscles 42.
Eccentric strengthening is currently the most commonly accepted therapeutic exercise approach for the treatment of tendinopathy 43. There have been case reports in the literature demonstrating improvement of proximal hamstring tendinopathy with eccentric exercises in athletes. Jayaseelan et al 44 described 2 cases of runners with proximal hamstring tendinopathy who were treated with eccentric hamstring loading, lumbopelvic stabilization exercises and trigger point needling. The athletes in both cases had significant improvements in pain and function over 8–10 weeks and returned to sport without pain 44. The beneficial effects of eccentric exercises have been attributed to the greater tendon load generated when compared to concentric exercises 45, increased collagen synthesis, decreased neovascularization, and force fluctuations from tendon loading and unloading. Options for eccentric hamstring exercises include hamstring curl machines, reverse cable curls, weight-bearing hamstring curls on an exercise ball, reverse planks, kneeling “Norwegian” (or “Nordic”) leg curls, and standing single- or double-leg dead lifts 38. It is typically recommended that eccentric exercises for the treatment of tendinopathy be performed at a level sufficient for the individual to feel discomfort of the tendon. However, the majority of hamstring exercises focus on resisted knee flexion, whereas runners primarily rely on hip extension, moreso than knee flexion, to increase their speed. Cushman et al 38 recently proposed an alternate method of hamstring eccentric strengthening using a treadmill, with the athlete standing backwards and eccentrically resisting movement of the belt (Figure 11).
The patient faced backward on a treadmill set at a speed of approximately 0.5 mi (0.8 km) per hour. He was instructed to hold onto the rails with both hands, with his uninvolved stationary limb placed off of the belt, while maintaining a neutral pelvic position. The hip of the involved limb was then extended while maintaining the knee extended, and the foot was placed on the belt behind the patient (Figure 11A). The patient then resisted the belt as it pulled his foot and limb forward, while maintaining a neutral pelvic posture (Figure 11B and C). When providing active resistance to the movement of the belt, the patient’s familiar buttock pain was reproduced as his hip moved toward flexion. The patient was therefore instructed to provide enough resistance to reproduce his typical pain to a moderate level (a numeric pain rating of between 4 and 6 on a 11-point scale) during exercise. He was also instructed to make sure that the pain did not get progressively worse or become disabling.
The patient immediately noted pain when performing this exercise, as compared to the lack of pain when performing the exercises assigned in the initial 4 weeks. He was instructed to perform this exercise 1 to 2 times daily for 3 sets of 12 to 15 repetitions. He was also asked to perform his plank exercises, progressing to contralateral single-leg/single-arm planks (eg, left arm on the floor and left leg raised off the floor) to be held for 30 seconds at a time and increasing to 60 seconds on each side. He also performed the double-leg, exercise-ball hamstring curls with the same number of sets and repetitions, progressing to unweighted, single-leg curls as an additional hamstring-strengthening exercise. He was permitted to do any of the other hamstring exercises and stretching, as an optional part of his regimen, but they were not mandatory.
Figure 11. Eccentric hamstring-strengthening exercise using the treadmill

Footnote: The treadmill is turned on to a slow speed, with the individual facing backward on the treadmill while holding on to the hand rails. The support side (the left leg, in this case) is placed off of the treadmill belt. (A) The involved leg (the right leg, in this case) is extended at the hip while keeping the knee mostly extended, and the individual is instructed to resist the forward motion of the belt with the leg. (B) The involved leg continues to actively resist the motion of the belt. (C) The involved leg continues to resist the belt before being repositioned to the starting point in (A).
[Source 46]Gluteal tendinopathy
Gluteal tendinopathy, often referred to as greater trochanteric bursitis or greater trochanteric pain syndrome, has a prevalence of 10-25% and is experienced by one in four women aged over 50 years 47. The disorder presents as pain and tenderness over the greater trochanter and often interferes with sleep and physical function. The level of disability and quality of life is equivalent to that of severe hip osteoarthritis 48 and effective management strategies are required.
Primary management of gluteal tendinopathy is conventional conservative management including rest, non-steroid anti-inflammatory drug, physiotherapy, and corticosteroid injection. In refractory cases, operative treatment such as lengthening of iliotibial band and fascia lata may be considered 49. Several studies reported extracorporeal shock wave therapy (ESWT) as a suitable alternative treatment option for refractory gluteal tendinopathy with satisfactory long-term maintenance 50. However, these studies included clinically diagnosed gluteal tendinopathy. Therefore, subjects with various conditions could be included, which alters the outcome, because accurate clinical diagnosis of gluteal tendinopathy is always difficult.
Figure 12. Gluteal tendinopathy MRI image
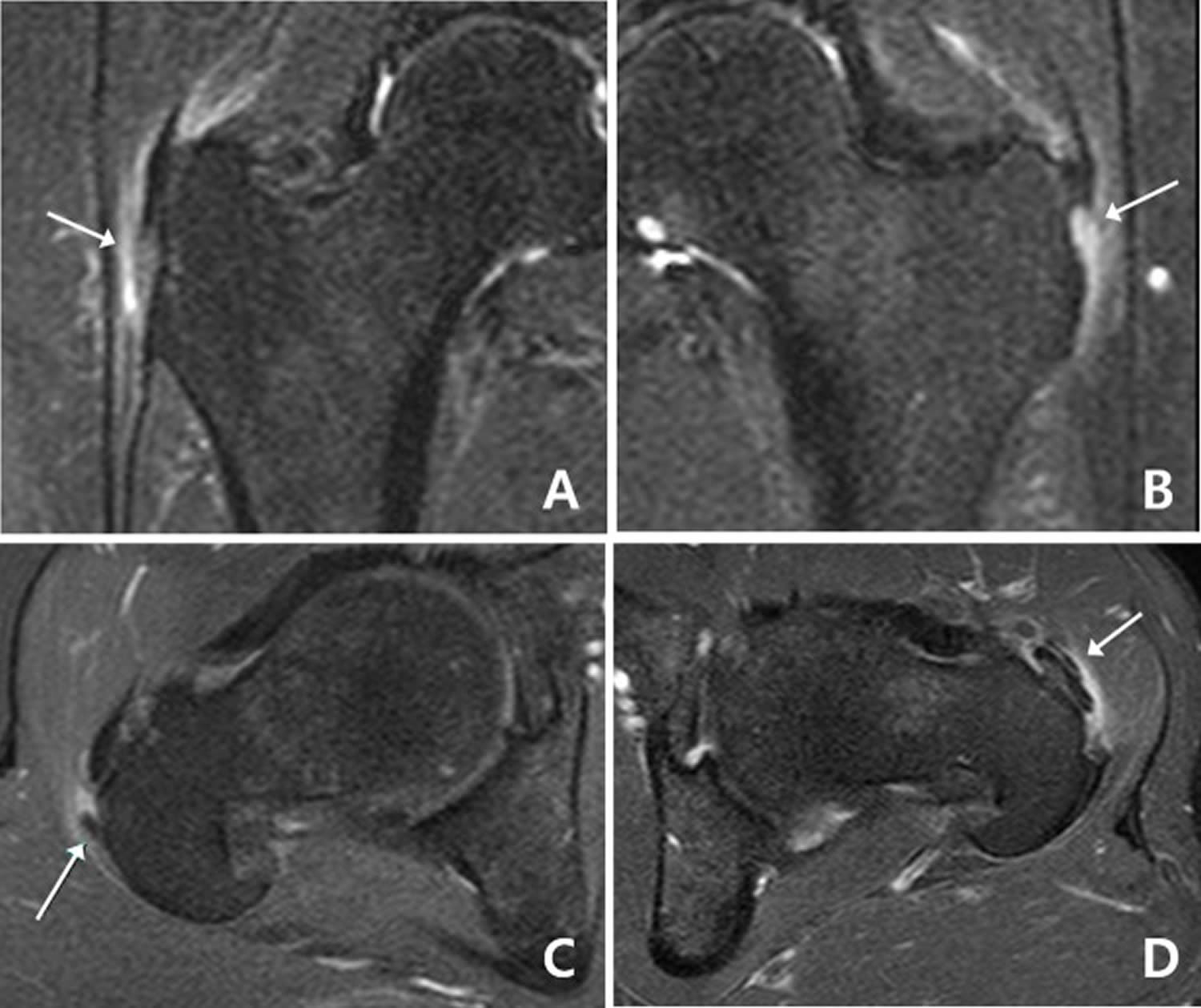
Footnote: A: Mild increased intrasubstance signal and surrounding edema (arrow) suggests gluteus medius tendinosis with peritendinitis. B: Marked increased intrasubstance signal and ill-definition of the gluteus medius tendon near the insertion on the lateral facet (arrow) suggests insertional partial tear. C: Contrast-enhanced axial T1 with fat saturation MR images demonstrates a hypointense calcium deposit (arrow) in the gluteus medius tendon with surrounding edema. D: Mild increased intrasubstance signal and surrounding edema (arrow) suggests gluteus minimus tendinosis with peritendinitis.
[Source 51]Tendinopathy treatment
Medical therapy
Nonsteroidal antiinflammatory medications
Oral nonsteroidal antiinflammatory medications (NSAIDS) have been used extensively for decades to treat pain associated with tendon overuse. More recently, the local administration of nonsteroidal antiinflammatory medications (NSAIDS) through gels or patches has been advocated. Literature search identified 37 randomized clinical trials and systematic reviews evaluating nonsteroidal antiinflammatory medications (NSAIDS) in the treatment of tendinopathy. Of these, only 17 studies were placebo-controlled 1. Overall, the evidence suggests both oral and local NSAIDS are effective in relieving the pain associated with tendinopathy in the short term (7–14 days) 1. Only three of the 17 studies evaluated showed no improvement with NSAIDS 1. Oral and local NSAIDs appear effective in the treatment of acute shoulder bursitis/tendonitis 1. One study also showed some success treating longer-standing shoulder pain with naprosyn sodium 52. In a randomized, placebo-controlled, double-blind study, naprosyn sodium was more effective than placebo but not as effective as a corticosteroid injection in the treatment of shoulder bursitis/tendonitis at 4 weeks. Not surprisingly, the patients who presented with a longer duration and greater severity of symptoms were more likely to have a poor response to both corticosteroid injection and/or oral NSAIDs.
NSAIDs do not seem nearly as effective in treating lateral epicondylitis (tennis elbow) or Achilles tendinopathy 53. The only study to look at the effectiveness of NSAIDS for the treatment of lateral epicondylitis (tennis elbow) in the long term reported no difference between placebo and naproxen treatment groups at 1-year followup 54. A systematic review of NSAID use for tennis elbow identified data to support the use of local NSAIDs with a decrease in pain in the short term (2 weeks) 55. However, there is little evidence to support or refute the use of topical or oral NSAIDs in the long term. In addition, long-term NSAID use increases the risk of gastrointestinal, cardiovascular, and renal complications associated with these medications. Overall, a short course of NSAIDs appears a reasonable option for the treatment of acute pain associated with tendon overuse, particularly about the shoulder. There is no clear evidence that NSAIDS are effective in the treatment of chronic tendinopathy in the long term.
Corticosteroid injections
Corticosteroid injections have been a mainstay in the treatment of tendinopathy 1. Despite their widespread use, there is some controversy as to their usefulness and safety in this setting. Literature search identified 19 controlled trials and systematic reviews with mixed results regarding corticosteroid injections in the treatment of tendinopathy 1. Several studies report good short-term pain control (≤ 6 weeks) with corticosteroid injections in patients with lateral epicondylitis and shoulder impingement 1. The long-term efficacy of corticosteroid injections for tendinopathy has not been demonstrated 1. Corticosteroid injections for lateral epicondylitis (tennis elbow) do not provide any long-term benefit (6–12 months) compared with placebo, NSAIDs, or physical therapy in randomized, controlled studies 54. Mixed results have been published with regard to the long-term benefits of subacromial corticosteroid injections for rotator cuff tendinopathy. Several well-controlled studies report a small but statistically significant level of improvement in the short term using corticosteroids in the treatment of shoulder impingement 56. In contrast, several authors have reported no major benefit with corticosteroid injections over control patients in the treatment of shoulder impingement 57. An extensive systematic review evaluating the efficacy of corticosteroid injections in the treatment of rotator cuff disease recently reported little or no evidence to support the use of corticosteroid injections for these patients 58.
In addition to the question of the efficacy of corticosteroid injections in the medium-term treatment of tendinopathy, there is a question of safety with using these medications in this setting. Several cases of Achilles tendon rupture have been reported after corticosteroid injections to this region 59. More recently, Gill et al. 60 described a series of 83 injections to the Achilles region without serious complication. The key point here is they injected the steroid under fluoroscopic guidance around the tendon but not within the substance of the tendon. Of note, only 40% of the patients in this series reported improvement after the procedure at the 2-year followup.
In summary, corticosteroid injections have been used for decades in the treatment of tendinopathy. There is strong evidence they relieve pain in the short term up to 6 weeks, but there is no evidence they provide any benefit in the long term (beyond 6 months) for the treatment of chronic tendinopathy. It appears the risks associated with corticosteroid injections can be minimized by injecting under image guidance to ensure the injection is paratendinous rather than intratendinous.
Glyceryl Trinitrate Patches
The treatment of tendinopathy with glyceryl trinitrate patches is an off-label use of an FDA-approved medication. Nitric oxide (NO) is a soluble molecule produced by a family of enzymes called nitric oxide synthases (NOS). In large doses, nitric oxide (NO) can be toxic, but in smaller, physiological doses, it acts as a cellular messenger and appears to play a role in blood pressure, memory, and host defense. Nitric oxide (NO) appears to play a role in tendon healing after injury. In a rat Achilles tendon healing model, inhibition of nitric oxide synthases (NOS) resulted in a decreased cross-sectional area and load to failure of the healing tendon 61. The addition of NO in this model enhances tendon healing suggesting the addition of exogenous NO to an area of tendon damage may promote tendon healing 62.
Based on this information, three randomized, controlled, double-blind clinical studies were designed to determine whether the topical administration of nitric oxide (NO) would enhance tendon healing in humans. In these studies, nitric oxide (NO) was delivered transcutaneously to the area of painful tendinopathy using commercially available glyceryl trinitrate (GTN) patches. This series of trials evaluated the effectiveness of the glyceryl trinitrate (GTN) patch in the treatment of lateral epicondylitis, Achilles tendinopathy, and rotator cuff tendinopathy 63. In all three studies, 53 to 86 patients were randomly assigned to the treatment group or control group. The treatment group received glyceryl trinitrate (GTN) patches that delivered 1.25 mg glyceryl trinitrate every 24 hours. The control group received a placebo patch. The patients and investigators were blinded to which patch was given to the patient. Both groups of patients were instructed to place the patch directly over the area of greatest tenderness/pain and to change the patch every 24 hours. The patches were worn until the symptoms subsided or the study ended (6 months).
All three studies showed improvement in the treatment groups compared with the control groups 1. In addition to decreased pain, patients demonstrated increased power and improved function in the area of interest. Most impressive was the percentage of patients who were asymptomatic with activities of daily living in the treatment group compared with the control group. In the tennis elbow study, 81% of the treatment group was asymptomatic compared with 60% of the control group. The Achilles tendinopathy study showed 78% of the treatment group asymptomatic with activities of daily living at 6 months versus 49% of the control group. Lastly, the supraspinatus tendinopathy data showed 46% of patients asymptomatic in the treatment group compared with 24% of the control subjects.
There is some question whether nitric oxide simply has an analgesic effect or a healing effect in the treatment of tendinopathy. A 3-year followup of the Achilles tendinopathy study described above has recently been published 64. It showed persistent improvement in the group treated with the glyceryl trinitrate patches for 6 months compared to the control group. At 3 years, 88% of the treatment group was completely asymptomatic compared to 67% of the control group. This study suggests treatment with transdermal glyceryl trinitrate had a healing effect rather than an analgesic effect in Achilles tendinopathy. In contrast to this, another randomized clinical trial was previously published comparing a 3-day course of transdermal nitroglycerin patches to placebo in 20 patients with rotator cuff tendinopathy 65. This study reported an improvement in pain scores in the treatment group compared to the control group as early as 24 hours after starting the patch. The improvement in pain was seen at all three time points: 1, 2, and 15 days. This suggests topical nitric oxide may have an analgesic effect as well.
As a whole, these studies provide convincing evidence the administration of NO directly over an area of tendinopathy through a glyceryl trinitrate patch enhances healing and provides some pain relief in the treatment of tendinopathy. The most commonly described side effect seen with this treatment modality is headaches 65. The headaches can be severe enough to cause cessation of treatment. As the majority of the work in the area of nitric oxide (NO) in the treatment of tendinopathy has come from one group, larger multicenter trials would be useful in validating this treatment modality.
Physical therapy
Physical therapy has been commonly used for the treatment of tendinopathies. There is, however, mixed data to support its use. The type of therapy used can be quite variable from one therapist to the next, and orthopaedic surgeons are often not involved in choosing the type of therapy used. Stretching and strengthening programs are a common component of most therapy programs. Therapists also use other modalities, including ultrasound, iontophoresis, deep transverse friction massage, low-level laser therapy, and hyperthermia.
Stretching/Strengthening
Eccentric strengthening programs have recently been advocated in the treatment of tendinopathy (Figure 9A–C) 66. Literature review identified 16 controlled clinical trials and systematic reviews evaluating this modality. One of these studies had a control group that received no treatment 67. This study showed improvement in the eccentric strengthening group compared to a “wait and see” group at 4 months 67. The other clinical trials evaluating eccentric strengthening compared it to other treatment modalities. A 12-week course of eccentric strengthening exercises was more effective than a traditional concentric strengthening program for treating Achilles and patellar tendinopathy in recreational athletes 68. In the Achilles tendinopathy study, 82% of the patients randomized to the eccentric strengthening protocol described improvement in pain levels compared with 36% in the concentric training group. Imaging of the Achilles tendon before and after a 12-week eccentric training protocol showed thinning and normalization of the tendon structure both on ultrasound and MRI 69. Interestingly, eccentric strengthening produced better results in tendinopathy of the midsubstance of the Achilles compared with insertional tendinopathy 70.
Eccentric strengthening protocols have also been successful in the treatment of lateral epicondylitis 71. In a well-designed study, 92 patients with lateral epicondylitis were randomized to a standard physical therapy protocol with and without an eccentric strengthening program 71. The group with the eccentric strengthening showed a considerable improvement in pain, strength, and function compared with the control group. A similar study showed no difference among patients assigned to stretching and icing alone, stretching and icing with eccentric strengthening, or stretching and icing with concentric strengthening 72. A systematic review of the literature on eccentric strength training for the treatment of tendinopathy has been published 73. Based on the variable results of the current studies, this review concluded there is only limited evidence to support the use of eccentric exercise over other treatments such as concentric exercise, stretching, splinting, massage, and ultrasound.
In addition to the data on eccentric strengthening, good results have been reported with a formal mobilization and strengthening program for rotator cuff tendonitis 74. In one study, 125 patients were randomized to arthroscopic acromioplasty, a formal supervised rotator cuff strengthening program, or a placebo laser treatment 75. Both the acromioplasty group and the physical therapy group had improved pain scores at 6 months compared with the placebo group. There was no difference in pain scores between the two treatment groups. In another randomized clinical trial, 52 patients with shoulder impingement were assigned to manual physical therapy in addition to a stretching and strengthening protocol or to stretching and strengthening without manual therapy 74. The study reported the addition of manual therapy resulted in an improvement in pain scores and strength at followup.
Other Modalities
There are a wide variety of modalities available to the physical therapist, and it is difficult to predict which technique or group of techniques a given therapist will utilize. While a typical orthopaedic surgeon is not involved in prescribing these treatments, it is worthwhile to have a feeling for what treatment options are available and how effective they are. Ultrasound, iontophoresis, low-level lasers, and phonophoresis are FDA approved; the 434-MHz hyperthermia device is not FDA approved for tendinopathy 1.
Literature review identified 51 references for clinical trials and systematic reviews of common therapy modalities. Low-level laser treatment has been studied extensively with mixed results 1. Of the 14 randomized clinical trials evaluating low-level laser treatment, two were discarded due to inadequate controls 1. Of the remaining studies, five showed improvement treating tendinopathy with low-level laser treatment compared to placebo low-level laser treatment, while seven studies showed no difference 1. Four systematic reviews have addressed low-level laser treatment and all agreed the best current level of evidence does not support its use in the treatment of tendinopathy 76.
The other physical therapy modalities have not been studied as extensively, but have similar conflicting results in the literature. Iontophoresis and phonophoresis involve using ionizing current or ultrasound to deliver medications locally. Corticosteroids and NSAIDS are commonly used with these modalities. Only six adequately controlled studies could be identified and four of these reported no improvement compared to controls 77. Transverse friction massage has also been used to treat tendinopathy, but only three studies have evaluated this modality 78. None of these studies showed a benefit to deep friction massage over other physical therapy modalities. A Cochrane review 78 evaluating deep friction massage found no benefit with deep friction massage over other treatments.
Another physical therapy modality commonly used in the treatment of tendinopathy is therapeutic ultrasound. Eight well-controlled trials and systematic reviews were identified on this subject. Three controlled trials demonstrated a benefit 79 with therapeutic ultrasound used in the treatment of lateral epicondylitis and calcific tendonitis of the supraspinatus. A systematic review of physical therapy modalities used for the treatment of shoulder pain suggested ultrasound appeared effective for the treatment of calcific tendonitis 80. Another extensive systematic review of the medical and physical therapy literature investigated the use of ultrasound for the treatment of musculoskeletal disorders 81. The only area where ultrasound showed slight promise was in the treatment of lateral epicondylitis. Pooled data from trials evaluating the treatment of lateral epicondylitis with ultrasound compared to controls showed the estimated difference in success rate to be 15% 81.
Hyperthermia has also been used in the treatment of tendinopathy. This modality involves using deep-heating machines that combine a superficial cooling system with a microwave-powered heating system. This can increase the temperature of target tissues approximately 4°C without damaging the skin. Presumably this increased temperature results in increased blood flow and subsequent healing to the damaged area. Two randomized clinical trials from a single institution have been published evaluating hyperthermia compared to therapeutic ultrasound in the treatment of tendinopathy 82. These trials report improvements in pain and patient satisfaction in the hyperthermia group compared to the ultrasound group. No other clinical trials have evaluated hyperthermia in the treatment of tendinopathy.
In summary, there is some evidence that eccentric strengthening programs may be effective in the treatment of tendinopathy. There is currently little evidence available to support the use of most physical therapy modalities including low-level laser treatment, iontophoresis, phonophoresis, therapeutic ultrasound, or deep friction massage 1. One exception to this is the use of ultrasound for calcific tendonitis. Early data on hyperthermia is also encouraging, but remains preliminary. Further research with higher-powered studies would be useful to determine the most effective physical therapy regime for the treatment of tendinopathies.
Shock-wave therapy
Extracorporeal shock wave therapy has been advocated for treating a number of soft tissue conditions, including plantar fasciitis, lateral epicondylitis, calcific and noncalcific tendonitis of the supraspinatus, and tendinopathy of the Achilles tendon 1. It is FDA-approved for plantar fasciitis and lateral epicondylitis only. extracorporeal shock wave therapy entails delivering a series of low-energy shock waves directly over the painful area of the tendon. The mechanism by which extracorporeal shock wave therapy would provide pain relief or enhance tendon healing is not clear.
The ideal method for applying extracorporeal shock wave therapy is also not clear. Published trials vary greatly with regard to the intensity and frequency of the shock waves, the duration of the treatment, the timing and number of repeat treatments given, and the use of local anesthetic. This variability makes it difficult to compare one study with the next.
In summary, extracorporeal shock wave therapy remains a controversial treatment option for tendinopathy. Good evidence is available to support the use of this modality in calcific tendinopathy of the rotator cuff. The best current evidence does not support its use in noncalcifying tendinopathy of the rotator cuff or lateral epicondylitis. Further evidence is needed to justify the use of extracorporeal shock wave therapy in Achilles tendinopathy and patellar tendinopathy. It is difficult to make conclusions with the current data available because of the wide variability in results and treatment protocols between studies.
Surgery
Surgery is often considered a last option in the treatment of tendinopathy that persists after exhausting all nonoperative options. The most commonly described procedure is open surgical débridement of the involved tendon or peritendinous tissue with repair or augmentation of the tendon as needed 1. Although good results can be obtained with débridement and/or decompression of chronic tendinopathies, these procedures are not without morbidity. Failure rates can be as high as 20% to 30% with some of these procedures, and it is difficult to predict who will have continued problems after surgery. For this reason, surgery remains the last option in the treatment of most cases of tendinopathy, and other options need to be explored.
Many studies evaluate various forms of surgery to treat Achilles tendinopathy. The approaches vary greatly between studies based partly on the extent of abnormality. Essentially all published studies of the surgical treatment of Achilles tendinopathy are retrospective in nature without control groups. The results vary between studies and appear to correlate with the extent of tendon damage. Morberg et al. 83 reported only a 67% satisfactory functional result at a mean followup of 6 years in a series of 64 patients who required débridement of devitalized tendon. Leppilahti et al. 84 reported 86% good to excellent results in treating patients with chronic peritendonitis, but only 69% good to excellent results when including the patients with substantial Achilles degeneration who underwent débridement of the tendon. Shepsis et al. showed similar results in 54 runners who underwent surgery for chronic Achilles pain 85. They reported satisfactory results in 87% of patients with paratendonitis and 67% in those with tendinosis.
Surgery has also been advocated for lateral epicondylitis that has failed nonoperative treatment 86. Nirschl and Pettrone described a 97.7% improvement rate with his open débridement procedure with 85.2% of patients returning to full activity 86. Since then, several reports have been published describing the results of open, arthroscopic, and percutaneous procedures for the treatment of lateral epicondylitis 87. Success rates in the 65% to 95% range have been reported, but all published reports have been retrospective or prospective case series without adequate controls. It is difficult to determine the best surgical approach for lateral epicondylitis because of the multitude of reports of different types of surgery that all seem to have moderately good results. A systematic review of surgical procedures for lateral epicondylitis reported in the Cochrane Database suggested no conclusions could be made because of the lack of controlled studies 88.
The results of surgical options for rotator cuff tendinopathy are also difficult to interpret. Rotator cuff tendinopathy of the shoulder is commonly believed the result of outlet impingement 89. Accordingly, open and/or arthroscopic acromioplasty have been the standard treatment for this condition if nonoperative measures have failed. Unless there is a partial- or full-thickness rotator cuff tear, the tendon itself is not addressed. Removing the bursa and impinging bone of the anterolateral acromion appears to provide good results in the vast majority of published trials 90. As mentioned earlier, the only randomized, placebo-controlled study to compare acromioplasty or supervised exercises to placebo in the treatment of shoulder impingement reported improvement in the surgery and exercise group compared to placebo 91. No difference was seen between the surgery and exercise groups.
There is not a great deal of evidence available regarding the best treatment once the tendon is degenerating and partially torn. Cordasco et al. showed good results with acromioplasty and débridement without rotator cuff repair in the treatment of articular-sided partial-thickness tears involving less than 50% of the tendon thickness 92. Interestingly, they did not see a progression to full-thickness tears in these patients up to 10 years after the procedure. In contrast, bursal-sided tears proved much more likely to progress to full-thickness lesions in this series. If the rotator cuff is partially torn involving more than 50% of its substance, the best available evidence supports repairing the torn tendon rather than simply débriding it and doing an acromioplasty 92. However, no prospective, randomized trials have been published looking at the results of repair versus débridement of partial-thickness rotator cuff tears.
Arthroscopic or open débridement of chronic calcific tendonitis also appears a good option if patients fail nonoperative treatment 93. Improvement in pain with a decrease in residual calcium deposits has been demonstrated after surgery compared with a matched cohort of patients treated nonoperatively 94. Surgical débridement of homogeneous calcium deposits in the supraspinatus appeared more reliable than extracorporeal shock wave therapy in a randomized, controlled trial 95. This treatment can be facilitated by marking the calcific deposits preoperatively using ultrasound guidance 96.
References- Andres BM, Murrell GAC. Treatment of Tendinopathy: What Works, What Does Not, and What is on the Horizon. Clinical Orthopaedics and Related Research. 2008;466(7):1539-1554. doi:10.1007/s11999-008-0260-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2505250/
- Mosca MJ, Rashid MS, Snelling SJ, Kirtley S, Carr AJ, Dakin SG. Trends in the theory that inflammation plays a causal role in tendinopathy: a systematic review and quantitative analysis of published reviews. BMJ Open Sport — Exercise Medicine. 2018;4(1):e000332. doi:10.1136/bmjsem-2017-000332. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6045756/
- Histopathology of common tendinopathies. Update and implications for clinical management. Khan KM, Cook JL, Bonar F, Harcourt P, Astrom M. Sports Med. 1999 Jun; 27(6):393-408. https://www.ncbi.nlm.nih.gov/pubmed/10418074/
- Neer Award 1999. Overuse activity injures the supraspinatus tendon in an animal model: a histologic and biomechanical study. Soslowsky LJ, Thomopoulos S, Tun S, Flanagan CL, Keefer CC, Mastaw J, Carpenter JE. J Shoulder Elbow Surg. 2000 Mar-Apr; 9(2):79-84. https://www.ncbi.nlm.nih.gov/pubmed/10810684/
- Rat supraspinatus tendon expresses cartilage markers with overuse. Archambault JM, Jelinsky SA, Lake SP, Hill AA, Glaser DL, Soslowsky LJ. J Orthop Res. 2007 May; 25(5):617-24.
- Patient education: Biceps tendinitis or tendinopathy (Beyond the Basics). https://www.uptodate.com/contents/biceps-tendinitis-or-tendinopathy-beyond-the-basics?view=print
- Biomechanics of tendon injury and repair. Lin TW, Cardenas L, Soslowsky LJ. J Biomech. 2004 Jun; 37(6):865-77.
- Identification of tendon stem/progenitor cells and the role of the extracellular matrix in their niche. Bi Y, Ehirchiou D, Kilts TM, Inkson CA, Embree MC, Sonoyama W, Li L, Leet AI, Seo BM, Zhang L, Shi S, Young MF. Nat Med. 2007 Oct; 13(10):1219-27
- Mechanisms of tendon injury and repair. Thomopoulos S, Parks WC, Rifkin DB, Derwin KA. J Orthop Res. 2015 Jun; 33(6):832-9.
- Chronic Achilles tendinopathy. A survey of surgical and histopathologic findings. Aström M, Rausing A. Clin Orthop Relat Res. 1995 Jul; (316):151-64.
- Effect of repetition rate on the formation of microtears in tendon in an in vivo cyclical loading model. Nakama LH, King KB, Abrahamsson S, Rempel DM. J Orthop Res. 2007 Sep; 25(9):1176-84.
- The pathobiology and repair of tendon and ligament injury. Goodship AE, Birch HL, Wilson AM. Vet Clin North Am Equine Pract. 1994 Aug; 10(2):323-49.
- Antioxidant enzyme peroxiredoxin 5 is upregulated in degenerative human tendon. Wang MX, Wei A, Yuan J, Clippe A, Bernard A, Knoops B, Murrell GA. Biochem Biophys Res Commun. 2001 Jun 15; 284(3):667-73.
- Oxidative energy metabolism in equine tendon cells. Birch HL, Rutter GA, Goodship AE. Res Vet Sci. 1997 Mar-Apr; 62(2):93-7.
- Arnoczky SP, Tian T, Lavagnino M, Gardner K, Schuler P, Morse P. Activation of stress-activated protein kinases (SAPK) in tendon cells following cyclic strain: the effects of strain frequency, strain magnitude, and cytosolic calcium. J Orthop Res. 2002;20(5):947–952.
- Skutek M, van Griensven M, Zeichen J, Brauer N, Bosch U. Cyclic mechanical stretching enhances secretion of interleukin 6 in human tendon fibroblasts. Knee Surg Sports Traumatol Arthrosc. 2001;9(5):322–326.
- Stone D, Green C, Rao U, et al. Cytokine-induced tendinitis: a preliminary study in rabbits. J Orthop Res. 1999;17(2):168–177.
- Frank C, McDonald D, Bray D, et al. Collagen fibril diameters in the healing adult rabbit medial collateral ligament. Connect Tissue Res. 1992;27(4):251–263.
- Lipman K, Wang C, Ting K, Soo C, Zheng Z. Tendinopathy: injury, repair, and current exploration. Drug Design, Development and Therapy. 2018;12:591-603. doi:10.2147/DDDT.S154660. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5865563/
- Shoulder Impingement/Rotator Cuff Tendinitis. http://orthoinfo.aaos.org/PDFs/A00032.pdf
- Tennis Elbow (Lateral Epicondylitis). http://orthoinfo.aaos.org/PDFs/A00068.pdf
- Proximal Biceps Tendonitis. https://kidshealth.org/en/teens/biceps-tendonitis.html
- De Quervain’s Tendinosis. http://orthoinfo.aaos.org/PDFs/A00007.pdf
- de Quervain’s Tenosynovitis. American Academy of Family Physicians. https://familydoctor.org/condition/de-quervains-tenosynovitis
- Jumper’s Knee. https://kidshealth.org/en/teens/jumpers-knee.html
- Irwin TA. Tendon injuries of the foot and ankle. In: Miller MD, Thompson SR, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 117.
- Biundo JJ. Bursitis, tendinitis, and other periarticular disorders and sports medicine. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 25th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 263.
- Yin MC, Ye J, Yao M, et al. Is extracorporeal shock wave therapy clinical efficacy for relief of chronic, recalcitrant plantar fasciitis? A systematic review and meta-analysis of randomized placebo or active-treatment controlled trials. Arch Phys Med Rehabil. 2014;95(8):1585-1593. PMID: 24662810 www.ncbi.nlm.nih.gov/pubmed/24662810
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360–366.
- CUSHMAN D, RHO ME. Conservative Treatment of Subacute Proximal Hamstring Tendinopathy Using Eccentric Exercises Performed With a Treadmill: A Case Report. The Journal of orthopaedic and sports physical therapy. 2015;45(7):557-562. doi:10.2519/jospt.2015.5762. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4615691/
- Miller SL, Webb GR. The proximal origin of the hamstrings and surrounding anatomy encountered during repair. Surgical technique. J Bone Joint Surg Am. 2008;90(suppl 2 pt 1):108–116. http://dx.doi.org/10.2106/JBJS.G.01281
- Fredericson M, Moore W, Guillet M, Beaulieu C. High hamstring tendinopathy in runners: meeting the challenges of diagnosis, treatment, and rehabilitation. Phys Sportsmed. 2005;33:32–43. http://dx.doi.org/10.3810/psm.2005.05.89
- Reliability and validity of three pain provocation tests used for the diagnosis of chronic proximal hamstring tendinopathy. Cacchio A, Borra F, Severini G, Foglia A, Musarra F, Taddio N, De Paulis F. Br J Sports Med. 2012 Sep; 46(12):883-7.
- Zissen MH, Wallace G, Stevens KJ, Fredericson M, Beaulieu CF. High hamstring tendinopathy: MRI and ultrasound imaging and therapeutic efficacy of percutaneous corticosteroid injection. AJR Am J Roentgenol. 2010;195:993–998. http://dx.doi.org/10.2214/AJR.09.3674
- De Smet AA, Blankenbaker DG, Alsheik NH, Lindstrom MJ. MRI appearance of the proximal hamstring tendons in patients with and without symptomatic proximal hamstring tendinopathy. AJR Am J Roentgenol. 2012;198:418–422. http://dx.doi.org/10.2214/AJR.11.6590
- Bowman KF, Jr, Cohen SB, Bradley JP. Operative management of partial-thickness tears of the proximal hamstring muscles in athletes. Am J Sports Med. 2013;41:1363–1371. http://dx.doi.org/10.1177/0363546513482717
- Shockwave therapy for the treatment of chronic proximal hamstring tendinopathy in professional athletes. Cacchio A, Rompe JD, Furia JP, Susi P, Santilli V, De Paulis F. Am J Sports Med. 2011 Jan; 39(1):146-53.
- Conservative Treatment of Subacute Proximal Hamstring Tendinopathy Using Eccentric Exercises Performed With a Treadmill: A Case Report. Cushman D, Rho ME. J Orthop Sports Phys Ther. 2015 Jul; 45(7):557-62.
- Fluoroscopically Guided Peritendinous Corticosteroid Injection for Proximal Hamstring Tendinopathy: A Retrospective Review. Nicholson LT, DiSegna S, Newman JS, Miller SL. Orthop J Sports Med. 2014 Mar; 2(3):2325967114526135.
- Wetzel RJ, Patel RM, Terry MA. Platelet-rich plasma as an effective treatment for proximal hamstring injuries. Orthopedics. 2013;36:e64–e70. http://dx.doi.org/10.3928/01477447-20121217-20
- White KE. High hamstring tendinopathy in 3 female long distance runners. J Chiropr Med. 2011;10:93–99. http://dx.doi.org/10.1016/j.jcm.2010.10.005
- Jayaseelan DJ, Moats N, Ricardo CR. Rehabilitation of proximal hamstring tendinopathy utilizing eccentric training, lumbopelvic stabilization, and trigger point dry needling: 2 case reports. J Orthop Sports Phys Ther. 2014;44:198–205. http://dx.doi.org/10.2519/jospt.2014.4905
- Kingma JJ, de Knikker R, Wittink HM, Takken T. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med. 2007;41:e3. http://dx.doi.org/10.1136/bjsm.2006.030916
- Rehabilitation of proximal hamstring tendinopathy utilizing eccentric training, lumbopelvic stabilization, and trigger point dry needling: 2 case reports. Jayaseelan DJ, Moats N, Ricardo CR. J Orthop Sports Phys Ther. 2014 Mar; 44(3):198-205.
- Stanish WD, Rubinovich RM, Curwin S. Eccentric exercise in chronic tendinitis. Clin Orthop Relat Res. 1986:65–68.
- CUSHMAN D, RHO ME. Conservative Treatment of Subacute Proximal Hamstring Tendinopathy Using Eccentric Exercises Performed With a Treadmill: A Case Report. The Journal of orthopaedic and sports physical therapy. 2015;45(7):557-562. doi:10.2519/jospt.2015.5762. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4615691
- Mellor R, Bennell K, Grimaldi A, et al. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. The BMJ. 2018;361:k1662. doi:10.1136/bmj.k1662. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5930290/
- Greater trochanteric pain syndrome negatively affects work, physical activity and quality of life: a case control study. Fearon AM, Cook JL, Scarvell JM, Neeman T, Cormick W, Smith PN. J Arthroplasty. 2014 Feb; 29(2):383-6.
- Management of the greater trochanteric pain syndrome: a systematic review. Del Buono A, Papalia R, Khanduja V, Denaro V, Maffulli N. Br Med Bull. 2012 Jun; 102():115-31.
- The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review. Mani-Babu S, Morrissey D, Waugh C, Screen H, Barton C. Am J Sports Med. 2015 Mar; 43(3):752-61.
- Seo K-H, Lee J-Y, Yoon K, et al. Long-term outcome of low-energy extracorporeal shockwave therapy on gluteal tendinopathy documented by magnetic resonance imaging. Nordez A, ed. PLoS ONE. 2018;13(7):e0197460. doi:10.1371/journal.pone.0197460. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6050036/
- Randomized, double-blind, placebo-controlled study of the treatment of the painful shoulder. Petri M, Dobrow R, Neiman R, Whiting-O’Keefe Q, Seaman WE. Arthritis Rheum. 1987 Sep; 30(9):1040-5.
- No effect of piroxicam on achilles tendinopathy. A randomized study of 70 patients. Aström M, Westlin N. Acta Orthop Scand. 1992 Dec; 63(6):631-4. https://www.ncbi.nlm.nih.gov/pubmed/1471511/
- Pragmatic randomised controlled trial of local corticosteroid injection and naproxen for treatment of lateral epicondylitis of elbow in primary care. Hay EM, Paterson SM, Lewis M, Hosie G, Croft P. BMJ. 1999 Oct 9; 319(7215):964-8.
- Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, Assendelft W. Cochrane Database Syst Rev. 2002; (2):CD003686.
- Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome? Akgün K, Birtane M, Akarirmak U. Clin Rheumatol. 2004 Dec; 23(6):496-500.
- A prospective, double-blind, randomized clinical trial comparing subacromial injection of betamethasone and xylocaine to xylocaine alone in chronic rotator cuff tendinosis. Alvarez CM, Litchfield R, Jackowski D, Griffin S, Kirkley A. Am J Sports Med. 2005 Feb; 33(2):255-62.
- The efficacy of subacromial corticosteroid injection in the treatment of rotator cuff disease: A systematic review. Koester MC, Dunn WR, Kuhn JE, Spindler KP. J Am Acad Orthop Surg. 2007 Jan; 15(1):3-11.
- Spontaneous rupture of the calcaneal tendon in rheumatoid arthritis after local steroid injection. Bedi SS, Ellis W. Ann Rheum Dis. 1970 Sep; 29(5):494-5.
- Fluoroscopically guided low-volume peritendinous corticosteroid injection for Achilles tendinopathy. A safety study. Gill SS, Gelbke MK, Mattson SL, Anderson MW, Hurwitz SR. J Bone Joint Surg Am. 2004 Apr; 86-A(4):802-6.
- Modulation of tendon healing by nitric oxide. Murrell GA, Szabo C, Hannafin JA, Jang D, Dolan MM, Deng XH, Murrell DF, Warren RF. Inflamm Res. 1997 Jan; 46(1):19-27.
- Addition of nitric oxide via nitroflurbiprofen enhances the material properties of early healing of young rat Achilles tendons. Yuan J, Murrell GA, Wei AQ, Appleyard RC, Del Soldato P, Wang MX. Inflamm Res. 2003 Jun; 52(6):230-7.
- Topical nitric oxide application in the treatment of chronic extensor tendinosis at the elbow: a randomized, double-blinded, placebo-controlled clinical trial. Paoloni JA, Appleyard RC, Nelson J, Murrell GA. Am J Sports Med. 2003 Nov-Dec; 31(6):915-20.
- Three-year followup study of topical glyceryl trinitrate treatment of chronic noninsertional Achilles tendinopathy. Paoloni JA, Murrell GA. Foot Ankle Int. 2007 Oct; 28(10):1064-8.
- Successful treatment of shoulder pain syndrome due to supraspinatus tendinitis with transdermal nitroglycerin. A double blind study. Berrazueta JR, Losada A, Poveda J, Ochoteco A, Riestra A, Salas E, Amado JA. Pain. 1996 Jul; 66(1):63-7.
- Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Am J Sports Med. 1998 May-Jun; 26(3):360-6.
- Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo Achillis: a randomized controlled trial. Rompe JD, Nafe B, Furia JP, Maffulli N. Am J Sports Med. 2007 Mar; 35(3):374-83.
- Superior results with eccentric compared to concentric quadriceps training in patients with jumper’s knee: a prospective randomised study. Jonsson P, Alfredson H. Br J Sports Med. 2005 Nov; 39(11):847-50.
- Eccentric training in patients with chronic Achilles tendinosis: normalised tendon structure and decreased thickness at follow up. Ohberg L, Lorentzon R, Alfredson H. Br J Sports Med. 2004 Feb; 38(1):8-11; discussion 11.
- Chronic Achilles tendon pain treated with eccentric calf-muscle training. Fahlström M, Jonsson P, Lorentzon R, Alfredson H. Knee Surg Sports Traumatol Arthrosc. 2003 Sep; 11(5):327-33.
- An isokinetic eccentric programme for the management of chronic lateral epicondylar tendinopathy. Croisier JL, Foidart-Dessalle M, Tinant F, Crielaard JM, Forthomme B. Br J Sports Med. 2007 Apr; 41(4):269-75.
- Chronic lateral epicondylitis: comparative effectiveness of a home exercise program including stretching alone versus stretching supplemented with eccentric or concentric strengthening. Martinez-Silvestrini JA, Newcomer KL, Gay RE, Schaefer MP, Kortebein P, Arendt KW. J Hand Ther. 2005 Oct-Dec; 18(4):411-9, quiz 420.
- Chronic tendinopathy: effectiveness of eccentric exercise. Woodley BL, Newsham-West RJ, Baxter GD. Br J Sports Med. 2007 Apr; 41(4):188-98; discussion 199.
- Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. Bang MD, Deyle GD. J Orthop Sports Phys Ther. 2000 Mar; 30(3):126-37.
- Arthroscopic surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome). Brox JI, Staff PH, Ljunggren AE, Brevik JI. BMJ. 1993 Oct 9; 307(6909):899-903.
- Physiotherapy interventions for shoulder pain. Green S, Buchbinder R, Hetrick S. Cochrane Database Syst Rev. 2003; (2):CD004258.
- Phonophoresis versus ultrasound in the treatment of common musculoskeletal conditions. Klaiman MD, Shrader JA, Danoff JV, Hicks JE, Pesce WJ, Ferland J. Med Sci Sports Exerc. 1998 Sep; 30(9):1349-55.
- Deep transverse friction massage for treating tendinitis. Brosseau L, Casimiro L, Milne S, Robinson V, Shea B, Tugwell P, Wells G. Cochrane Database Syst Rev. 2002; (1):CD003528.
- Is therapeutic ultrasound effective in treating soft tissue lesions? Binder A, Hodge G, Greenwood AM, Hazleman BL, Page Thomas DP. Br Med J (Clin Res Ed). 1985 Feb 16; 290(6467):512-4.
- Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for shoulder pain. Philadelphia Panel. Phys Ther. 2001 Oct; 81(10):1719-30.
- Ultrasound therapy for musculoskeletal disorders: a systematic review. van der Windt DA, van der Heijden GJ, van den Berg SG, ter Riet G, de Winter AF, Bouter LM. Pain. 1999 Jun; 81(3):257-71.
- Hyperthermia at 434 MHz in the treatment of overuse sport tendinopathies: a randomised controlled clinical trial. Giombini A, Di Cesare A, Casciello G, Sorrenti D, Dragoni S, Gabriele P. Int J Sports Med. 2002 Apr; 23(3):207-11.
- Long-term results after surgical management of partial Achilles tendon ruptures. Morberg P, Jerre R, Swärd L, Karlsson J. Scand J Med Sci Sports. 1997 Oct; 7(5):299-303.
- Overuse injuries of the Achilles tendon. Leppilahti J, Orava S, Karpakka J, Takala T. Ann Chir Gynaecol. 1991; 80(2):202-7.
- Surgical management of Achilles tendon overuse injuries. A long-term follow-up study. Schepsis AA, Wagner C, Leach RE. Am J Sports Med. 1994 Sep-Oct; 22(5):611-9.
- Tennis elbow. The surgical treatment of lateral epicondylitis. Nirschl RP, Pettrone FA. J Bone Joint Surg Am. 1979 Sep; 61(6A):832-9.
- Percutaneous release of the common extensor origin for tennis elbow. Grundberg AB, Dobson JF. Clin Orthop Relat Res. 2000 Jul; (376):137-40.
- Surgery for lateral elbow pain. Buchbinder R, Green S, Bell S, Barnsley L, Smidt N, Assendelft WJ. Cochrane Database Syst Rev. 2002; (1):CD003525.
- Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. Neer CS 2nd. J Bone Joint Surg Am. 1972 Jan; 54(1):41-50.
- High patient satisfaction after arthroscopic subacromial decompression for shoulder impingement: a prospective study of 50 patients. Bengtsson M, Lunsjö K, Hermodsson Y, Nordqvist A, Abu-Zidan FM. Acta Orthop. 2006 Feb; 77(1):138-42.
- Arthroscopic surgery compared with supervised exercises in patients with rotator cuff disease (stage II impingement syndrome) Brox JI, Staff PH, Ljunggren AE, Brevik JI. BMJ. 1993 Oct 9; 307(6909):899-903.
- The partial-thickness rotator cuff tear: is acromioplasty without repair sufficient? Cordasco FA, Backer M, Craig EV, Klein D, Warren RF. Am J Sports Med. 2002 Mar-Apr; 30(2):257-60.
- Prospective randomized surgical treatments for calcifying tendinopathy. Rubenthaler F, Ludwig J, Wiese M, Wittenberg RH. Clin Orthop Relat Res. 2003 May; (410):278-84.
- Surgical or conservative treatment for chronic rotator cuff calcifying tendinitis–a matched-pair analysis of 100 patients. Wittenberg RH, Rubenthaler F, Wölk T, Ludwig J, Willburger RE, Steffen R. Arch Orthop Trauma Surg. 2001; 121(1-2):56-9.
- Shock wave therapy versus conventional surgery in the treatment of calcifying tendinitis of the shoulder. Rompe JD, Zoellner J, Nafe B. Clin Orthop Relat Res. 2001 Jun; (387):72-82.
- Value of preoperative ultrasound marking of calcium deposits in patients who require surgical treatment of calcific tendinitis of the shoulder. Kayser R, Hampf S, Seeber E, Heyde CE. Arthroscopy. 2007 Jan; 23(1):43-50.





{kind=link}