
What is thoracentesis
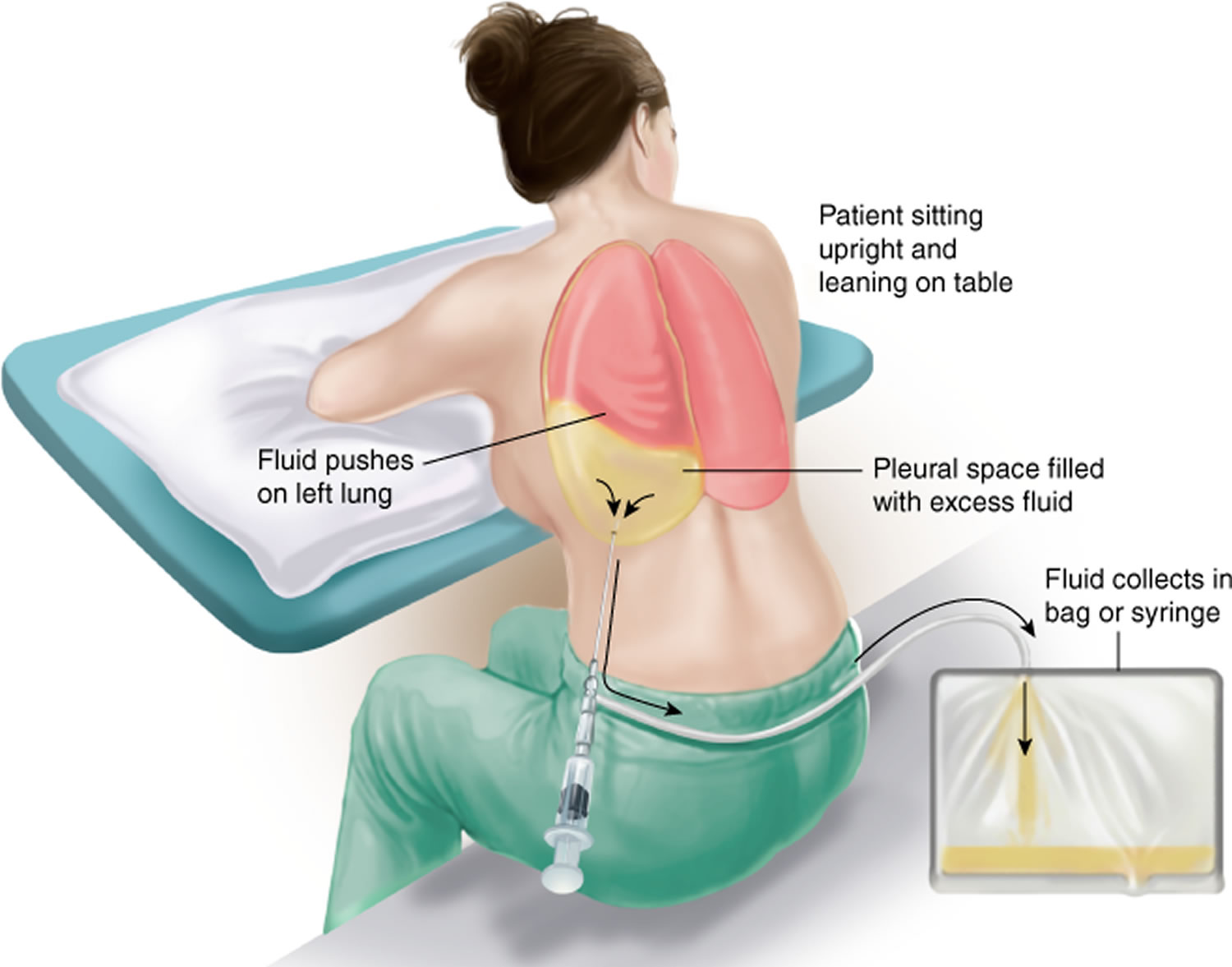
Thoracentesis or pleural tap, is a procedure in which a needle is inserted into the pleural space between the lungs and the chest wall to remove excess fluid, known as a pleural effusion, from the pleural space to help you breathe easier. Normally the pleural cavity contains only a very small amount of fluid. Thoracentesis may be done to determine the cause of your pleural effusion. Pleural effusion is one of the major causes of pulmonary mortality and morbidity 1.
Pleural effusion is the most common disease among all the pleural disease and affects 1.5 million patients per year in the United States 2. A wide variety of diseases can present with pleural effusions like diseases primarily involving the lung like pneumonia, asbestos exposure, primarily systemic diseases like lupus, rheumatoid arthritis, or maybe the pleural manifestation of diseases which primarily affect other organs like congestive heart failure, pancreatitis, or diseases local to the pleura like pleural infections and mesothelioma 3.
Testing the pleural fluid will help your doctor determine the cause of your pleural effusion. Possible causes include:
- Cancer
- Liver failure
- Heart failure
- Low protein levels
- Kidney disease
- Trauma or post-surgery
- Asbestos-related pleural effusion
- Collagen vascular disease (class of diseases in which the body’s immune system attacks its own tissues)
- Drug reactions
- Collection of blood in the pleural space (hemothorax)
- Lung cancer
- Swelling and inflammation of the pancreas (pancreatitis)
- Pneumonia
- Blockage of an artery in the lungs (pulmonary embolism)
- Severely underactive thyroid gland
If your doctor suspects that you have an infection, a culture of the fluid may be done to test for bacteria.
Thoracentesis is performed in a doctor’s office or hospital. Thoracentesis procedure usually takes 10 to 15 minutes, unless you have a lot of fluid in your pleural space. For the procedure, most patients sit quietly on the edge of a chair or bed with their head and arms resting on a table. Your doctor may use ultrasound to determine the best location to insert the needle. After cleaning the skin around the area where the needle will be inserted, your doctor will inject numbing medicine. A needle is inserted between your ribs into the pleural space. You may feel some discomfort or pressure when the needle is inserted. As your doctor draws out excess fluid from around your lungs, you may feel like coughing or have chest pain. The needle will be removed, and a small bandage will be applied to the site.
After the procedure, your blood pressure and breathing will be monitored to make sure you do not have complications. The fluid that was removed from your chest will be sent for laboratory testing to determine the cause of your pleural effusion and to help plan your treatment. Your doctor may order a chest x ray to check for lung problems.
The risks of thoracentesis include a pneumothorax or collapsed lung, pain, bleeding, bruising, or infection. Liver or spleen injuries are rare complications.
Management-tip
- Known transudative effusions do not require thoracentesis unless they are very large or causing unmanageable dyspnea.
- Uncomplicated parapneumonic effusions typically resolve with medical management without thoracentesis.
- Complicated parapneumonic effusions require thoracentesis to prevent the formation of scars (pleural “peels”) heralding lung trapping and loss of function.
Thoracentesis indications
Normally, very little fluid is in the pleural space. A buildup of too much fluid between the layers of the pleura is called a pleural effusion. The indications for thoracentesis are relatively broad including diagnostic and therapeutic clinical management 4. Thoracentesis is commonly performed to determine the cause of the extra fluid in the pleural space or to relieve symptoms from the fluid buildup.
Thoracentesis should be performed diagnostically whenever the excessive fluid is of unknown cause. Thoracentesis also should be performed therapeutically when the volume of fluid is causing significant clinical symptoms 5.
Typically diagnostic thoracentesis is small volume (single 20cc to 30cc syringe). Unless the cause is obvious, a first-time thoracentesis should have a diagnostic sample collected for laboratory and pathology analysis.
Typically, therapeutic thoracentesis is large volume (multiple liters of fluid). A small sample of a large volume thoracentesis should be sent for analysis when the etiology of the fluid is unknown or there is a question of a change in the etiology (e.g., new infection, decompensated chronic condition).
If the volume of fluid is anticipated to reaccumulate quickly, a drain is often left in place to collect this fluid. This often is seen in trauma (e.g., hemothorax), cancer (e.g., malignant effusion), post-operatively (e.g., cardiothoracic post-operative healing/inflammatory conditions), and end-stage metabolic conditions with the systemic excessive colloid leak (e.g., cirrhosis or malabsorption syndromes).
A fluid collection that is believed to be infected should be drained to eliminate the source of infection and/or reservoirs of the infection.
Thoracentesis contraindications
There are no absolute contraindications for thoracentesis 5.
Relative contraindications include any condition in which the potential risk of the thoracentesis procedure is greater than the probable benefit. Common potential risks include coagulopathy, overlying skin/soft-tissue infection, anatomical variants including congenital defects deforming identifiable anatomy, acquired anatomical variants such as pleural adhesions, and collections of fluid that are unlikely to be aspirated via needle drainage such as a loculated effusion.
Thoracentesis procedure
The thoracentesis procedure is done in the following way:
- You sit on a bed or on the edge of a chair or bed. Your head and arms rest on a table.
- The skin around the procedure site is cleaned. A local numbing medicine (anesthetic) is injected into the skin. 1% lidocaine and a needle to inject anesthetic (25 gauge for the skin and a slightly larger needle for the soft tissue). Administer local anesthesia to the skin (25 gauge needle to make a wheal at the surface of the skin) and soft tissue. After the local anesthetic is administered, use a larger, 22 gauge, needle to infiltrate the tissue around the rib, marching the needle tip just above the rib margin.
- A needle or catheter attached to a syringe or the prepackaged catheter directly perpendicular to the skin and muscles of the chest wall into the space around the lungs, called the pleural space. Your health care provider may use ultrasound to find the best spot to insert the needle.
- Needle or IV catheter for fluid aspiration – If using a prepared kit, this will consist of a plastic sheath cannula attached to a syringe. If a kit is not being used, a spinal needle should be used (18g or 20g). IV needles are inappropriate due to their short length and the thin wall of the sheath that will collapse under the surrounding soft tissue.
- Stop-cock to allow sealed start/stop collection of fluid and to divert fluid for sampling into a separate syringe
- Syringe (20-60cc size is appropriate) to collect a sample of fluid
- IV tubing
- Sterile fluid collection container suitable for the laboratory
- The fluid may be sent to a laboratory for testing (pleural fluid analysis).
- Post-procedure dressing – Gauze and tape or bandaid are sufficient.
No special preparation is needed before the test. A chest x-ray or ultrasound will be done before and after the thoracentesis procedure.
DO NOT cough, breathe deeply, or move during the test to avoid injury to the lung.
You will feel a stinging sensation when the local anesthetic is injected. You may feel pain or pressure when the needle is inserted into the pleural space.
Tell your provider if you feel short of breath or have chest pain.
Tips
- If flow stops after started, have the patient Valsalva or cough to increase intrathoracic pressure and improve flow.
- If the patient develops hypotension, respiratory distress, a rapid drop in oxygen saturation, or you see air bubbles in the syringe, obtain an immediate chest radiograph and prepare for management of a pneumothorax.
- When removing the needle, having the patient Valsalva will decrease the risk of pneumothorax at the time of needle withdrawal. Obtain a chest radiograph after the procedure to monitor change in fluid level and screen for Pneumothorax
Thoracentesis location
The preferred site for the procedure is on the affected side in either the midaxillary line if the procedure is being performed in the supine position or the posterior midscapular line if the procedure is being performed in the upright or seated position.
Bedside ultrasound should be used to identify an appropriate location for the procedure. Placing the patient in the upright seated position and using bedside ultrasound can aid in identifying fluid pockets in patients with lower fluid volumes.
Ultrasound can confirm the presence of fluid and identify an area with a sufficient amount of fluid for aspiration, thereby decreasing the incidence of both unsuccessful aspiration and complications. Ultrasound increases the success rate of thoracentesis and helps to prevent an unnecessary invasive procedure in some patients. Ultrasound also is useful to identify soft tissue rib landmark anatomy when these landmarks are difficult to identify by palpation due to body habitus.
If an ultrasound machine is not available, percussion technique on physical exam may be used to find the fluid level. Generally, entering between the seventh and ninth ribs will minimize the risk of complication and increase the likelihood of success.
Thoracentesis position
Thoracentesis is done in either a supine or sitting position depending on patient comfort, underlying condition, and the clinical indication 6.
Thoracentesis complications
Complications include bleeding, pain, and infection at the point of needle entry. Complications also can occur from the traumatic introduction of a sharp needle into the soft tissues of the chest wall (e.g., intercostal neurovascular bundle) and deeper thoracic structures (e.g., pneumothorax, pericardial injury, myocardial puncture, or cardiac arteries), and subphrenic solid organ injury (e.g., splenic or hepatic puncture) 5. However, when done with care, thoracentesis has no complications in most patients. To reduce the risk of complications, use of ultrasound is useful, especially when the fluid collection is small or loculated 6.
For large volume thoracentesis (greater than 500mL), hypotension or re-expansion pulmonary edema are potential complications 5. If a large pleural effusion is drained quickly and volumes of more than 1.5 liter are removed, the rapid re-expansion of the collapsed lung may occasionally lead to re-expansion pulmonary edema. Pleural manometry and monitoring pleural pressure during drainage of large volumes and terminating further drainage once the pleural pressure drops below -20 cm water or terminating with the onset of chest pain may prevent re-expansion pulmonary edema 2.
Thoracentesis fluid
Pleural fluid is a liquid derived from the blood in the tiny blood vessels (capillaries) in the lungs. It is found in small quantities between the layers of the pleurae – membranes that cover the chest cavity and the outside of each lung. It serves as a lubricant for the movement of the lungs during breathing. In the normal healthy adult, the pleural cavity has minimal fluid which acts a lubricant for the two pleural surfaces. The amount of pleural fluid is around at 0.1 ml/kg to 0.3 ml/kg and is constantly exchanged 2. Pleural fluid originates from the vasculature of parietal pleura surfaces and is absorbed back by lymphatics in the dependent diaphragmatic and mediastinal surfaces of parietal pleura. Hydrostatic pressure from the systemic vessels that supply the parietal pleura is thought to drive the interstitial fluid into the pleural space and hence has a lower protein content than serum. Accumulation of excess fluid can occur if there is excessive production or decreased absorption or both overwhelming the normal homeostatic mechanism. If pleural effusion is mainly due to mechanisms that lead to pleural effusion mainly due to increased hydrostatic pressure are usually transudative, and leading to pleural effusion have altered the balance between hydrostatic and oncotic pressures (usually transudates), increased mesothelial and capillary permeability (usually exudates) or impaired lymphatic drainage 7
A variety of conditions and diseases can cause inflammation of the pleurae (pleuritis) and/or excessive accumulation of pleural fluid (pleural effusion). Pleural fluid analysis is a group of tests that evaluate this liquid to determine the cause of the increased fluid.
The two main reasons for fluid accumulation in the pleural space are:
- An imbalance between the pressure of the liquid within blood vessels, which drives fluid out of blood vessels, and the amount of protein in blood, which keeps fluid in blood vessels. The fluid that accumulates in this case is called a transudate. This type of fluid more commonly involves both sides of the chest and is most frequently a result of either congestive heart failure or cirrhosis.
- An injury to or inflammation of the pleurae, in which case the fluid that accumulates is called an exudate. It more commonly involves one side of the chest and may be seen in infections (pneumonia, tuberculosis), malignancies (lung cancer, metastatic cancer, lymphoma, mesothelioma), or other causes of inflammation (sarcoidosis, autoimmune diseases).
Determining the type of fluid present is important because it helps to shorten the list of possible causes of pleural effusion. Healthcare practitioners and laboratorians use an initial set of tests (cell count, protein, albumin, and lactate dehydrogenase (LDH) level, and appearance of the fluid) to distinguish between transudates and exudates. If the fluid is an exudate, additional tests may be performed to further pinpoint the disease or condition causing pleuritis and/or pleural effusion.
Light criteria can be used to determine if the fluid is an exudate versus transudate 8.
Note: A blood glucose, protein, albumin, or LDH may be ordered to compare concentrations with those in the pleural fluid.
To be an exudate, the pleural effusion must have at least one of the following:
- Pleural fluid/serum LDH ratio > 0.6, or LDH > 2/3 the upper limit of normal, or
- Pleural fluid/serum total protein ratio > 0.5.
Transudate
Approximately 90% are from congestive heart failure, and the remaining 10% are caused by hepato-hydrothorax, nephrotic syndrome, peritoneal dialysis, myxedema, atelectasis, constrictive pericarditis, SVC syndrome, and hypoalbuminemia.
Exudate
Low glucose (glucose < 60 or ratio fluid/serum < 0.5), complicated parapneumonic effusion versus empyema, tuberculosis (TB), malignancy, vasculitis (i.e., lupus), esophageal rupture (Tip: rheumatoid or empyema glucose often < 10).
Common causes of exudates include pulmonary infections like pneumonia or tuberculosis, malignancy, inflammatory disorders like pancreatitis, lupus, rheumatoid arthritis, post-cardiac injury syndrome, chylothorax (due to lymphatic obstruction), hemothorax (blood in pleural space) and benign asbestos pleural effusion.
Some of the less common causes of pleural effusion are a pulmonary embolism which can be exudate or transudate, drug-induced (e.g., methotrexate, amiodarone, phenytoin, dasatinib, usually exudate), post-radiotherapy (exudate), esophageal rupture (exudate) and ovarian hyperstimulation syndrome (exudate).
Initial test results may include:
- Physical characteristics—fluid may appear cloudy
- Protein, albumin, or LDH level—high
- Cell count—increased
Low pH (pH < 7.2)
Complicated parapneumonic effusion versus empyema, tuberculosis, malignancy, vasculitis (i.e., lupus), esophageal rupture, hemothorax, or parasitic (Tip: esophageal rupture often < 6).
Bloody (red blood cells > 100K)
Due to trauma, malignancy, pulmonary embolism, infarction, tuberculosis, or post-operative.
Cell Count high Lymphocytes
As in lymphoma, malignancy not otherwise specified, tuberculosis, fungal, or post-operative.
Thoracentesis fluid analysis
Thoracentesis fluid analysis is used to help diagnose the cause of accumulation of fluid in the chest cavity (pleural effusion). There are two main reasons for fluid accumulation and an initial set of tests, including fluid protein, albumin, or LDH level, cell count, and appearance, is used to differentiate between the two types of fluid that may be produced, transudate or exudate.
Transudate
An imbalance between the pressure within blood vessels (which drives fluid out of the blood vessel) and the amount of protein in blood (which keeps fluid in the blood vessel) can result in accumulation of fluid. Transudates are most frequently caused by congestive heart failure or cirrhosis. If the fluid is determined to be a transudate, then usually no more tests on the fluid are necessary.
Transudates are most often caused by either congestive heart failure or cirrhosis. Typical fluid analysis results include:
- Physical characteristics—fluid appears clear
- Protein, albumin, or LDH level—low
- Cell count—few cells are present
Exudate
Injury or inflammation of the pleurae may cause abnormal collection of fluid. If the fluid is an exudate, then additional testing is often ordered. Exudates are associated with a variety of conditions and diseases, including:
- Infectious diseases – caused by viruses, bacteria, or fungi. Infections may originate in the pleurae or spread there from other places in the body. For example, pleuritis and pleural effusion may occur along with or following pneumonia.
- Bleeding – bleeding disorders, pulmonary embolism, or trauma can lead to blood in the pleural fluid.
- Inflammatory conditions – such as lung diseases, chronic lung inflammation for example due to prolonged exposure to large amounts of asbestos (asbestosis), sarcoidosis, or autoimmune disorders such as rheumatoid arthritis and lupus
- Malignancies – such as lymphoma, leukemias, lung cancer, metastatic cancers
- Other conditions – idiopathic, cardiac bypass surgery, heart or lung transplantation, pancreatitis, or intra-abdominal abscesses
Additional testing on exudate fluid may include:
- Pleural fluid glucose, lactate, amylase, triglyceride, and/or tumor markers
- Microscopic examination – a laboratory professional may place a sample of the fluid on a slide and examine it under a microscope. Normal pleural fluid has small numbers of white blood cells (WBCs) but no red blood cells (RBCs) or microorganisms.
- Cytology – a laboratory professional may use a special centrifuge (cytocentrifuge) to concentrate the fluid’s cells on a slide. The slide is treated with a special stain and evaluated for abnormal cells, such as malignant cells (cancer cells).
- Gram stain – for direct observation of bacteria or fungi under a microscope. There should be no organisms present in pleural fluid.
- Bacterial culture and susceptibility testing – ordered to detect any bacteria that may be present in the pleural fluid and to guide antimicrobial therapy.
- Fungal tests – may include fungal culture and susceptibility testing
- Adenosine deaminase – may help detect tuberculosis (TB)
- Less commonly, tests for infectious diseases, such as tests for viruses, mycobacteria (AFB testing), and parasites.
Additional test results and their associated causes may include:
Physical characteristics – the normal appearance of a sample of pleural fluid is usually light yellow and clear. Abnormal results may give clues to the conditions or diseases present and may include:
- Reddish pleural fluid may indicate the presence of blood.
- Cloudy, thick pleural fluid may indicate an infection and/or the presence of white blood cells. It may also indicate leakage of fluid from the lymphatic system (lymph). Lymph drains from the lymphatic system into the venous system in the chest and either trauma or lymphoma can cause lymph to be present in pleural fluid.
Chemical tests – tests that may be performed in addition to protein or albumin may include:
- Glucose—typically about the same as blood glucose levels; may be lower with infection and rheumatoid arthritis.
- Lactate levels can increase with infections.
- Amylase levels may increase with pancreatitis, esophageal rupture, or malignancy.
- Triglyceride levels may be increased when there is leakage from the lymphatic system.
- Tumor markers, such as CEA, may be increased with some cancers.
Microscopic examination – Normal pleural fluid has small numbers of white blood cells (WBCs) but no red blood cells (RBCs) or microorganisms. Results of an evaluation of the different kinds of cells present may include:
- Total cell counts—the white blood cells and red blood cells in the sample are counted. Increased white blood cells may be seen with infections and other causes of pleuritis. Increased red blood cells may suggest trauma, malignancy, or pulmonary infarction.
- White blood cell differential—determination of percentages of different types of white blood cells. An increased number of neutrophils may be seen with bacterial infections. An increased number of lymphocytes may be seen with cancers and tuberculosis.
- Cytology—a cytocentrifuged sample is treated with a special stain and examined under a microscope for abnormal cells. This is often done when a mesothelioma or metastatic cancer is suspected. The presence of certain abnormal cells, such as tumor cells or immature blood cells, can indicate what type of cancer is involved.
Infectious disease tests – these tests may be performed to look for microorganisms if infection is suspected:
- Gram stain—for direct observation of bacteria or fungi under a microscope. There should be no organisms present in pleural fluid.
- Bacterial culture and susceptibility testing—If bacteria are present, susceptibility testing can be performed to guide antimicrobial therapy. If there are no bacteria present, it does not rule out an infection; they may be present in small numbers or their growth may be inhibited because of prior antibiotic therapy.
- Fungal tests—if a culture is positive, the fungus or fungi causing the infection will be identified in the report and susceptibility testing may be done to guide therapy.
- Adenosine deaminase—a markedly elevated level in pleural fluid in a person with symptoms that suggest tuberculosis means it is likely that the person tested has a Mycobacterium tuberculosis infection in their pleurae. This is especially true when there is a high prevalence of tuberculosis in the geographic region where a person lives.
Other less common tests for infectious diseases may be performed and may identify a virus, mycobacteria (such as the mycobacterium that causes tuberculosis), or a parasite as the cause of an infection and fluid accumulation.
When is thoracentesis fluid analysis ordered?
Pleural fluid analysis may be ordered when a healthcare practitioner suspects that a person has a condition or disease that is causing pleuritis and/or pleural effusion. It may be ordered when someone has some combination of the following signs and symptoms:
- Chest pain that worsens with deep breathing
- Coughing
- Difficulty breathing, shortness of breath
- Fever, chills
- Fatigue
Treatment of pleural effusion
Once the cause of pleural effusion is determined, management involves addressing the underlying cause. In cases of complex parapneumonic effusions or empyema, (pleural fluid pH less than 7.2 or presence of organisms) chest tube drainage is usually indicated along with antibiotics. Small-bore drains (10 G to 14 G) are equally effective as large bore drains for this purpose 2. If patients do not respond to appropriate antibiotics and adequate drainage, then thoracoscopic decortication or debridement may be necessary. Instillation of intrapleural fibrinolytics and DNAse may be used to improve drainage and in those who do not respond to sufficient antibiotic therapy and those who are not candidates for surgical intervention.
If a patient with malignant pleural effusion is not symptomatic, drainage is not always indicated unless an underlying infection is suspected. For malignant pleural effusions that require frequent drainage, options for management are pleurodesis (where the pleural space is obliterated either mechanically or chemically by inducing irritants into the pleural space) and tunneled pleural catheter placement 9.
Thoracentesis recovery time
The outcome of patients with pleural effusions depends on the cause, severity and patient comorbidity 2. In general, people who do not seek therapy have a poor outcome compared to those who are treated. Overall, patients with malignant pleural effusions tend to have a poor outcome. Most patients are dead within 12-24 months, irrespective of the cause of the malignant pleural effusion 2. When pleural effusions are inadequately treated, this can result in an empyema, sepsis and even a trapped lung 10.
References- Kugasia IAR, Kumar A, Khatri A, Saeed F, Islam H, Epelbaum O. Primary effusion lymphoma of the pleural space: Report of a rare complication of cardiac transplant with review of the literature. Transpl Infect Dis. 2018 Oct 01;:e13005
- Krishna R, Rudrappa M. Pleural Effusion. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448189
- Dancel R, Schnobrich D, Puri N, Franco-Sadud R, Cho J, Grikis L, Lucas BP, El-Barbary M, Society of Hospital Medicine Point of Care Ultrasound Task Force. Soni NJ. Recommendations on the Use of Ultrasound Guidance for Adult Thoracentesis: A Position Statement of the Society of Hospital Medicine. J Hosp Med. 2018 Feb;13(2):126-135.
- Terra RM, Dela Vega AJM. Treatment of malignant pleural effusion. J Vis Surg. 2018;4:110.
- Wiederhold BD, O’Rourke MC. Thoracentesis. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441866
- Alzghoul B, Innabi A, Subramany S, Boye B, Chatterjee K, Koppurapu VS, Bartter T, Meena NK. Optimizing the Approach to Patients With Pleural Effusion and Radiologic Findings Suspect for Cancer. J Bronchology Interv Pulmonol. 2018 Jul 25
- Arnold DT, De Fonseka D, Perry S, Morley A, Harvey JE, Medford A, Brett M, Maskell NA. Investigating unilateral pleural effusions: the role of cytology. Eur. Respir. J. 2018 Nov;52,5
- Lepus CM, Vivero M. Updates in Effusion Cytology. Surg Pathol Clin. 2018 Sep;11(3):523-544
- Bueno Fischer G, Teresinha Mocelin H, Feijó Andrade C, Sarria EE. When should parapneumonic pleural effusions be drained in children? Paediatr Respir Rev. 2018 Mar;26:27-30.
- Iyer NP, Reddy CB, Wahidi MM, Lewis SZ, Diekemper RL, Feller-Kopman D, Gould MK, Balekian AA. Indwelling Pleural Catheter versus Pleurodesis for Malignant Pleural Effusions: A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018 Oct 01





{kind=link}