
Triangular alopecia
Triangular alopecia also known as triangular temporal alopecia, congenital temporal alopecia or Brauer nevus, is a non-scarring form of hair loss (alopecia) usually seen on the frontotemporal scalp 1, although there have been reported cases of congenital triangular alopecia affecting the temporoparietal 2 and occipital scalp 3. Temporal triangular alopecia was first described in 1905 by Raymond Sabouraud in his book “Manuel élémentaire de dermatologie topographique réégionale” as “alopecia triangulare congenitale de la temp” 4. Triangular temporal alopecia most commonly presents in children aged 2–9 years, although it can be present at birth or may first appear in adult life. It affects both men and women and is more commonly seen in light-skinned people.
Temporal triangular alopecia is a nonprogressive disorder, which presents as a triangular, oval or lancet-shaped patch of alopecia 5. Congenital triangular alopecia is usually unilateral but may be bilateral in up to 20% of cases 5. Congenital temporal alopecia may manifest at birth or develop in adulthood 6. Triangular alopecia remains unchanged throughout the life 7. There is no gender predilection 8. The incidence in the general population is estimated to be 0.11% 1. Most of the reported cases were in Caucasian patients, although congenital triangular alopecia has also been documented among Asians 9 and African-Americans 10. In a published series of 53 patients by Yamazaki et al. 11 in 2010, more than ½ (58.8%) of the cases appeared in patients between the ages of two and nine, while over a third (36.5%) manifest at birth and 3.8% presented in adulthood. From a literature review 12, 79% of patients with congenital triangular alopecia presented with unilateral hair loss while 18.5% of patients had bilateral involvement. About 2.5% consulted with occipital alopecia and 51.6% of the patients were male, versus 48.4% of females. These figures are consistent with previously published data. Many believe temporal triangular alopecia is under-reported due to affected individuals not presenting with symptoms. Misdiagnosis of triangular temporal alopecia as alopecia areata, male pattern alopecia, traction alopecia, trichotillomania, or congenital aplasia cutis would also contribute to the impression of rarity.
Congenital triangular alopecia is often asymptomatic and remains unchanged throughout the life; it is viewed as a permanent condition with no specific treatment necessary except for cosmetic reasons. The exact nature of congenital triangular alopecia should be explained to parents so that they can avoid fruitless investigations or harmful treatments 8. Medical treatment of congenital triangular alopecia with topical or intralesional corticosteroids have not proved effective 13. Bang et al. 9 reported a successful case of transient improvement with the use of 3% topical minoxidil in a 1-year-old child. Terminal hair growth was observed. Unfortunately, hair regrowth was not sustained following the cessation of treatment. Hair restoration surgery using follicular unit transplantation or surgical excision may provide patients with a satisfactory cosmetic result 14. Long-term sustained benefits have been reported after 6 years of follow-up 15.
Figure 1. Triangular temporal alopecia

Footnote: Congenital triangular alopecia affecting the frontotemporal regions bilaterally in an 8-year-old girl (left frontotemporal hair loss shown in this photograph)
[Source 12 ]Triangular temporal alopecia causes
The cause of triangular temporal alopecia is unknown. Once considered congenital (present at birth), congenital triangular alopecia appears to be acquired in the majority of individuals 16. Temporal triangular alopecia usually appears sporadically but has been reported to run in families, suggesting a possible genetic link 17. Triangular temporal alopecia has been reported in a number of genetic conditions, including Down syndrome and phacomatosis pigmentovascularis.
It has been postulated that congenital triangular alopecia may reflect mosaicism 2 and may be inherited as a paradominant trait where a postzygotic loss of the wild type allele in a heterozygote state leads to disease 18. Others have suggested that congenital triangular alopecia may be an ectodermal defect and should be included in the group of epidermal nevus 17. There is currently no consensus, and the exact cause of temporal triangular alopecia is unclear. There appears to be no obvious phylogenetic or embryological explanation for congenital triangular alopecia 7. Nonetheless, the development of congenital triangular alopecia in the first year of life in an area of the scalp that had previously appeared normal is strongly indicative of a localized process of miniaturization of the hair follicles, which produces regression to vellus hair 9. The stimulus responsible for this irreversible regression remains unknown.
Table 1. Reported disorders presenting in association with congenital triangular alopecia
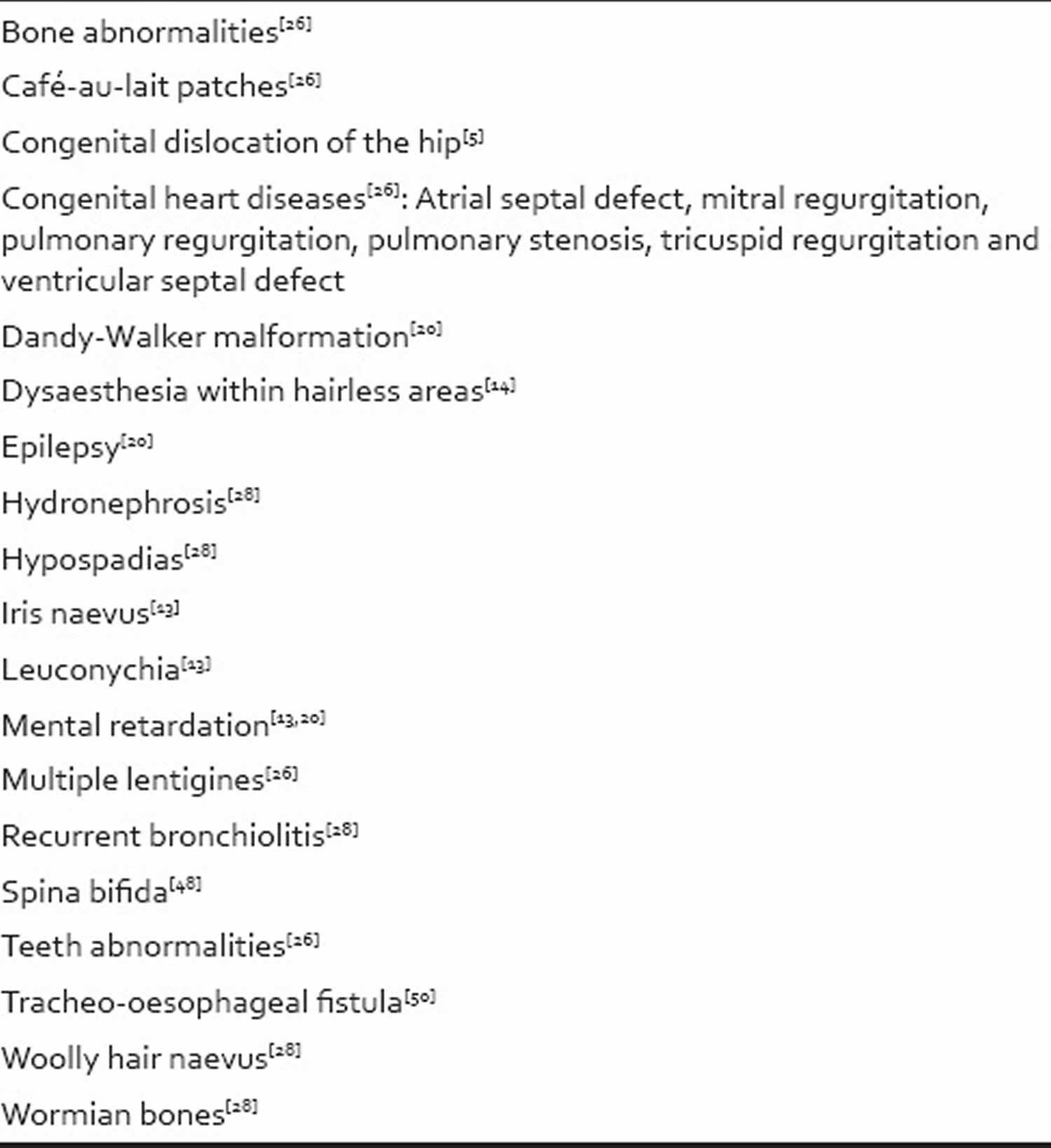
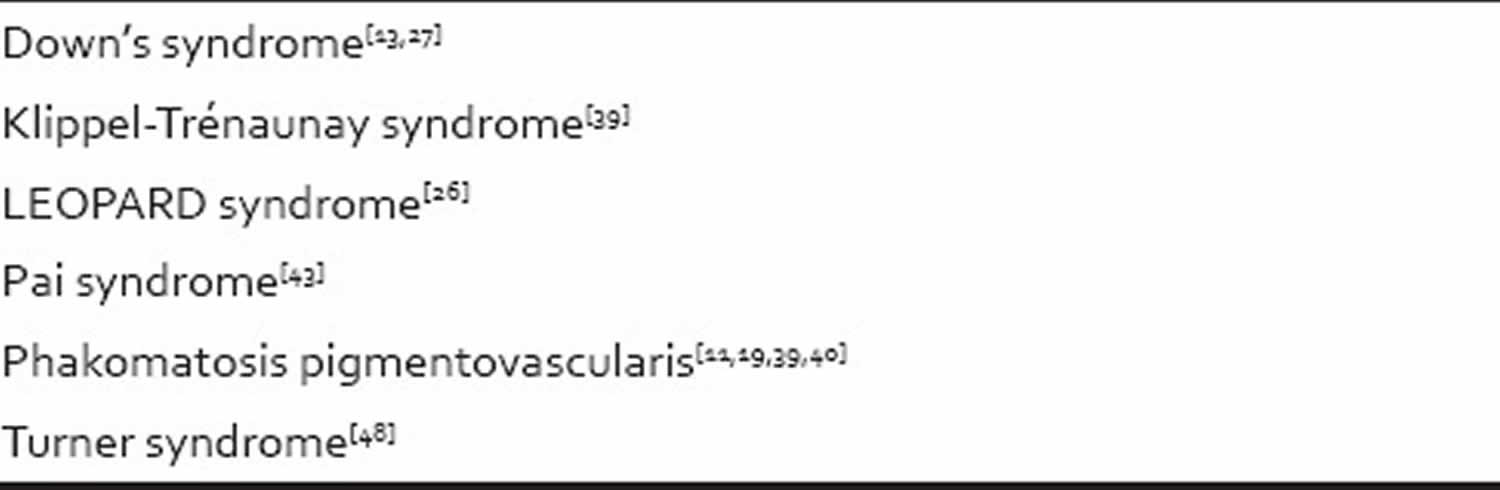
Table 2. Reported syndromes associated with congenital triangular alopecia
Triangular temporal alopecia differential diagnosis
Sometimes, congenital triangular alopecia may be misdiagnosed as other types of localized alopecia that present with a small, round or oval hairless patch in atypical locations on the scalp. Common differential diagnoses of congenital triangular alopecia include 12:
- Alopecia areata
- Alopecia mucinosa
- Androgenetic alopecia
- Aplasia cutis
- Primary cicatricial alopecia
- Pressure alopecia
- Tinea capitis
- Traction alopecia
- Trichotillomania
- Sebaceous nevus
Triangular temporal alopecia signs and symptoms
Triangular temporal alopecia appears as a triangular or spear-shaped loss of hair, with the ‘point’ of the triangle directed up and back. The shape is sometimes round or oval. It usually does not cause any symptoms, but sometimes patients report dysaesthesia in the lesion.
The lesion most commonly appears on the temporal scalp on one side only, although can affect both sides. Involvement of the occipital hairline has also been reported.
Temporal triangular alopecia often has a fringe of terminal hairs (mature adult hair) along the frontal hairline and sometimes also a tuft of hair within the lesion 19 or as small islands of dark hairs 20. Vellus hairs (soft finer hair) are seen throughout the area.
Kubba and Rook 7 noted that in the vast majority of cases the area of alopecia was not noted by a child’s parents until after 3 years of age. This latency period is attributed to the relatively sparse pelage during the 1st year of life 5. Parents may only become aware of the affected patch when it contrasts significantly with the surrounding hair, as the vellus hairs are replaced by terminal hair 7.
The lesion remains unchanged throughout life. Despite the presence of vellus hairs, there is no hair regrowth. There are no clinical signs of inflammation or scarring.
Triangular temporal alopecia diagnosis
The diagnosis of triangular temporal alopecia is usually clinical and based on its distinct clinical appearance and location.
Trichoscopic examination using a handheld polarized light dermatoscope has emerged as a helpful diagnostic tool as it can help to elucidate clinical signs that cannot be recognized by the naked eye 21. Dermoscopy can distinguish triangular temporal alopecia from alopecia areata and male pattern alopecia. The dermoscopic features to look for are the presence of vellus hairs throughout the lesion with terminal hairs at the edge. There is no inflammation or scarring. The ‘exclamation mark’ hairs (short broken off hairs that resemble an exclamation mark), yellow dots, and black dots of alopecia areata are not present, nor are the ‘streamers’ (residual fibrovascular tracts) of male pattern alopecia. The presence of epidermal scaling, as well as interfollicular features such as arborizing red lines and a honeycomb pigment pattern, may also be useful clues 21. Vellus hairs are a highly sensitive but not specific marker for congenital triangular alopecia 21. A study by Shim et al. 22 demonstrated clustered short vellus hairs without other specific findings. Videodermoscopy has also been used 23. The hair pull test was negative in all reported cases 21.
A skin biopsy is not usually required, but histology shows a normal number of hair follicles in the superficial dermis, mainly of the vellus type.
A classification system for the diagnosis of congenital triangular alopecia proposed by Inui et al. 24 emphasized the importance of four main clinical features. Suggested criteria for diagnosis include:
- A triangular or spear-shaped patch of hair loss located over the frontotemporal region of the scalp
- Dermoscopy revealing normal follicle openings with vellus hairs surrounded by normal terminal hairs
- Dermoscopy showing no yellow and black dots, dystrophic hairs (hairs that are bent at the skin layer or fractured or exclamation mark hairs) with a preserved follicular openings
- No significant hair regrowth 6 months after confirming the presence of vellus hairs on dermoscopy.
Histology
In congenital triangular alopecia, normal terminal hair follicles are typically replaced by sparse vellus hair follicles 25. The total number of hair follicle units are usually in the normal range 9, except for an isolated case report of a decreased number of hair follicles 26. The epidermis and dermis are unremarkable 6 with no evidence of an inflammatory infiltrate 16. However, hair follicles are miniaturized 2 with an increased proportion of vellus or indeterminate hairs 27. This may be due to abnormalities in follicle morphogenesis and supports the idea that congenital triangular alopecia is a form of a hamartomatous mosaic disease possibly involving an abnormal, local, epithelial-mesenchymal interaction 11. Collagen bundles and vessels in the dermis shows no abnormalities; sweat glands and sebaceous glands are normal in size and number 11. Bacterial and fungal stains are negative 6.
Triangular alopecia treatment
Congenital triangular alopecia is often asymptomatic and remains unchanged throughout the life; it is likely that many patients do not consult a physician for this particular condition 28. Temporal triangular alopecia treatment is generally not required and is mostly ineffective. Surgical excision of the lesion, if the lesion is small, or hair transplants, if cosmetically significant, have been used successfully.
References- García-Hernández MJ, Rodríguez-Pichardo A, Camacho F. Congenital triangular alopecia (Brauer nevus) Pediatr Dermatol. 1995;12:301–3.
- Tas B, Pilanci Ö, Basaran K. Congenital temporal triangular alopecia: A typical Brauer nevus. Acta Dermatovenerol Alp Pannonica Adriat. 2013;22:93–4.
- Bonifazi E. Hypotrichotic nevus (congenital triangular alopecia) Eur J Pediatr Dermatol. 2011;21:57.
- Sabouraud R. A Manual of Regional Topographical Dermatology. Paris: Masson; 1905. p. 197.
- Trakimas C, Sperling LC, Skelton HG, 3rd, Smith KJ, Buker JL. Clinical and histologic findings in temporal triangular alopecia. J Am Acad Dermatol. 1994;31:205–9.
- Trakimas CA, Sperling LC. Temporal triangular alopecia acquired in adulthood. J Am Acad Dermatol. 1999;40:842–4.
- Kubba R, Rook A. Congenital triangular alopecia. Br J Dermatol. 1976;95:657–9.
- León-Muiños E, Monteagudo B, Labandeira J, Cabanillas M. Bilateral congenital triangular alopecia associated with congenital heart disease and renal and genital abnormalities. Actas Dermosifiliogr. 2008;99:578–9.
- Bang CY, Byun JW, Kang MJ, Yang BH, Song HJ, Shin J, et al. Successful treatment of temporal triangular alopecia with topical minoxidil. Ann Dermatol. 2013;25:387–8.
- Erickson Q, Yanase D, Perry V. Temporal triangular alopecia: Report of an African-American child with TTA misdiagnosed as refractory tinea capitis. Pediatr Dermatol. 2002;19:129–31.
- Yamazaki M, Irisawa R, Tsuboi R. Temporal triangular alopecia and a review of 52 past cases. J Dermatol. 2010;37:360–2.
- Yin Li VC, Yesudian PD. Congenital Triangular Alopecia. Int J Trichology. 2015;7(2):48-53. doi:10.4103/0974-7753.160089 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4502474
- Jiménez-Acosta F, Ponce I. Hair transplantation in triangular temporal alopecia. Actas Dermosifiliogr. 2009;100:913–5.
- Chung J, Sim JH, Gye J, Namkoong S, Hong SP, Kim MH, et al. Successful hair transplantation for treatment of acquired temporal triangular alopecia. Dermatol Surg. 2012;38:1404–6.
- Unger R, Alsufyani MA. Bilateral temporal triangular alopecia associated with phakomatosis pigmentovascularis type IV successfully treated with follicular unit transplantation. Case Rep Dermatol Med. 2011;2011:129541.
- Kudligi C, Bhagwat PV, Eshwarrao MS, Tandon N. Giant congenital triangular alopecia mimicking alopecia areata. Int J Trichology. 2012;4:51–2.
- Patrizi A, Morrone P, Fiorentini C, Bianchi T. An additional familial case of temporal triangular alopecia. Pediatr Dermatol. 2001;18:263–4.
- Happle R. Congenital triangular alopecia may be categorized as a paradominant trait. Eur J Dermatol. 2003;13:346–7.
- Assouly P, Happle R. A hairy paradox: Congenital triangular alopecia with a central hair tuft. Dermatology. 2010;221:107–9.
- Bargman H. Congenital temporal triangular alopecia. Can Med Assoc J. 1984;131:1253–4.
- Karadag Köse O, Güleç AT. Temporal triangular alopecia: Significance of trichoscopy in differential diagnosis. J Eur Acad Dermatol Venereol. 2014 doi: 10.1111/jdv.12656
- Shim WH, Jwa SW, Song M, Kim HS, Ko HC, Kim BS, et al. Dermoscopic approach to a small round to oval hairless patch on the scalp. Ann Dermatol. 2014;26:214–20.
- Iorizzo M, Pazzaglia M, Starace M, Militello G, Tosti A. Videodermoscopy: A useful tool for diagnosing congenital triangular alopecia. Pediatr Dermatol. 2008;25:652–4.
- Inui S, Nakajima T, Itami S. Temporal triangular alopecia: Trichoscopic diagnosis. J Dermatol. 2012;39:572–4.
- Minars N. Congenital temporal alopecia. Arch Dermatol. 1974;109:395–6.
- Silva CY, Lenzy YM, Goldberg LJ. Temporal triangular alopecia with decreased follicular density. J Cutan Pathol. 2010;37:597–9.
- Oliveira LC, Miranda AR, Pinto SA, Ianhez M. Case for diagnosis. Alopecia areata and congenital triangular alopecia. An Bras Dermatol. 2014;89:353–5.
- Tosti A. Congenital triangular alopecia. Report of fourteen cases. J Am Acad Dermatol. 1987;16:991–3.





{kind=link}