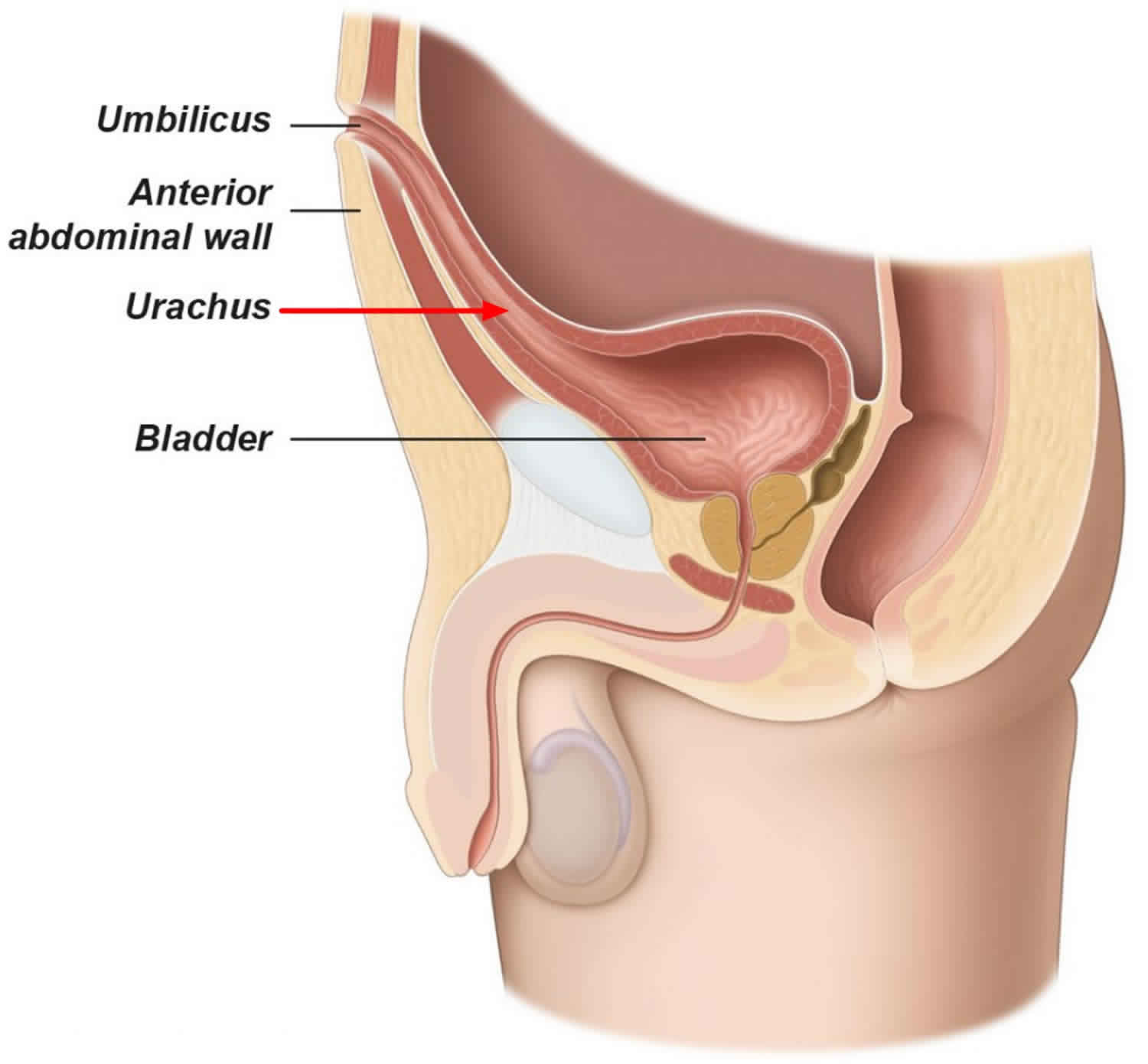
What is urachus
Urachus is a tube-like structure that connects the umbilical cord (belly button) to the urinary bladder that is present before birth, which goes away before birth. After birth, the lumen of the urachus usually shrinks into a small median umbilical ligament, a midline linear fibrous fold of parietal peritoneum, extending from the apex of the bladder to the umbilicus. But sometimes part of the urachus remains after birth. It is unclear why this happens.
If the lumen of the urachus does not completely involute, a spectrum of urachal remnants may persist, including:
- Patent urachus is commonest (~50%) communication between the bladder and umbilicus through a urachus that has not involuted
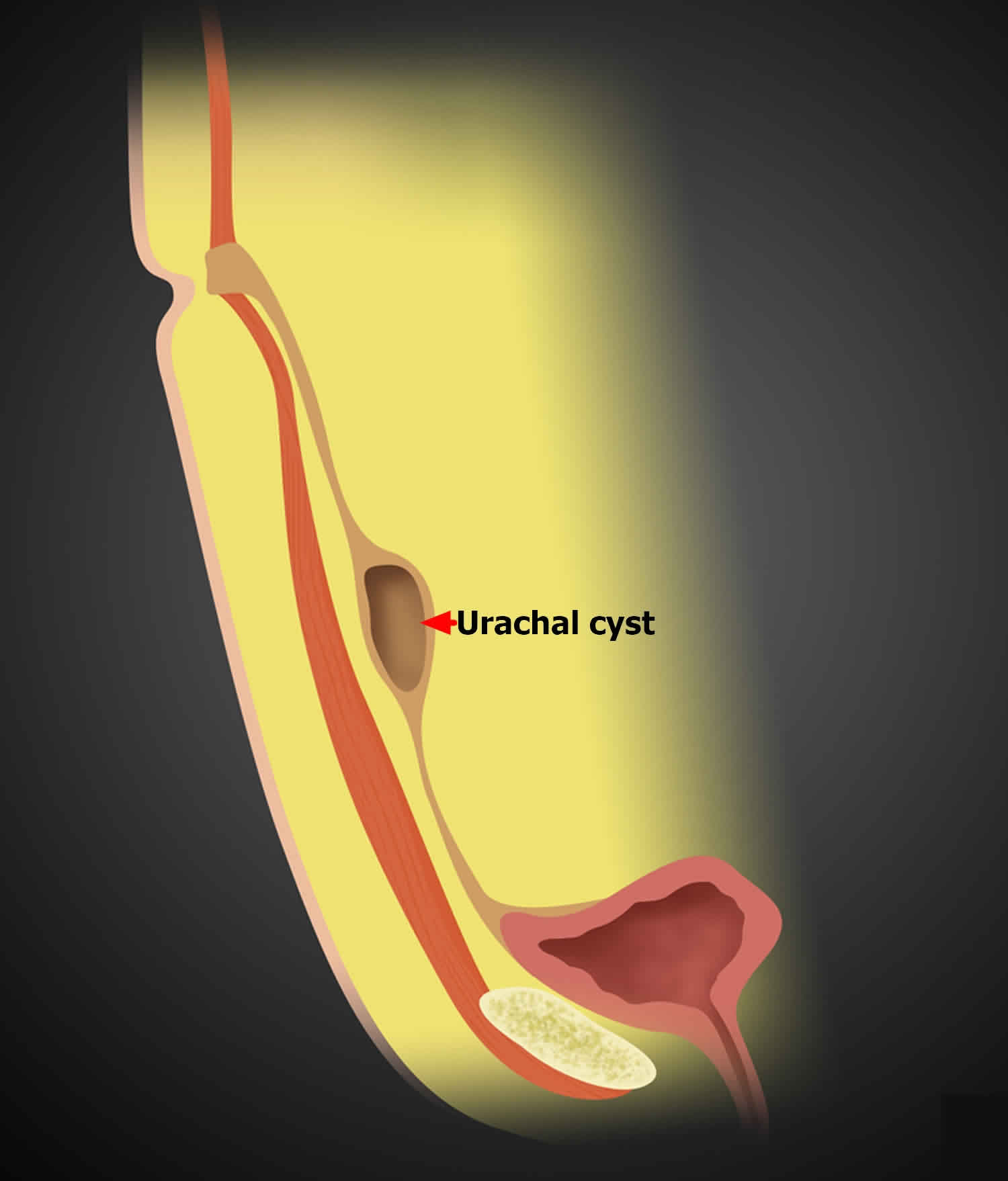
- Urachal cyst next commonest (~30%), is a fluid-filled dilatation of the mid urachus
- Urachal-umbilical sinus about ~15%, is a blind focal dilatation of the umbilical end of the urachus
- Vesico-urachal diverticulum about ~5%, is a blind focal dilatation of the bladder end of the urachus
A urachal remnant may develop adenocarcinoma.
Urachus is usually diagnosed in early infancy. The urachus has no purpose after birth, so if it remains it can cause health problems. These problems are called “urachal abnormalities.” Problems with a urachal abnormality are rare. They can be seen in infants or children, and rarely in adults. The incidence of a patent urachus is approximately 1 in 70 000 in the general population 1. Traces of the urachus called “urachal residues”, can be detected in up to one-third of adults. Urachal residues usually do not cause any symptoms.
Figure 1. Patent urachus
What happens under normal conditions?
As a baby develops, the urinary bladder is formed in the lower belly of the growing fetus. The urinary bladder is joined with the umbilical cord by a thick cord called the urachus. After the first few weeks of growth, this thick path to and from the placenta has blood vessels, a channel (that will later become the intestine), and a tube called the allantois. The inside of the allantois is joined to the top of the growing bladder. This link from the top of the bladder to the belly button is formed in about 20 weeks.
Because the urachus is found between the belly button and the top of the bladder, diseases of the urachus can appear anywhere in that space.
Urachal cyst
Urachal cysts form when both the umbilical and vesical ends of the urachal lumen close while an intervening portion remains patent and fluid filled. The cyst can drain through the umbilicus, bladder, or through the peritoneum and into intraperitoneal organs. Rarely it can cause peritonitis and abdominal symptoms. Urachal cysts usually remain asymptomatic until complicated by infection or bleeding. An infected urachal cyst can occur at any age. The most common pathogens of urachal abscess are Staphylococcus, E. coli, Pseudomonas, and Streptococcus.
An uncomplicated urachal cyst appears as a collection of simple fluid localized in the midline of the anterior abdominal wall, between the umbilicus and the pubis and often contiguous with the bladder dome.
Treatment of a urachal cyst may involve IV antibiotic therapy and/or surgical excision. Drainage is usually associated with a high rate of relapse. Sometimes it is advisable to drain the cyst contents before its excision.
Figure 2. Urachal cyst
Umbilical-urachal sinus
An umbilical-urachal sinus represents a non-communicating dilatation of the urachus at the umbilical end.
Umbilical-urachal sinus clinical presentation is commoner in children and rare in adult.
An umbilical-urachal sinus can manifest at ultrasound as a thickened tubular structure along the midline below the umbilicus.
Umbilical-urachal sinus complications
- infection, with possible abscess formation
- concurrent occurrence of a tumor.
Figure 3. Urachal-umbilical sinus

Vesico-urachal diverticulum
Vesico-urachal diverticulum is the proximal equivalent of a urachal umbilical sinus, representing a result of the failure of the urachus to close at the urinary bladder, forming an out-pouching of variable length from the anterosuperior aspect of the urinary bladder, which does not communicate with the umbilicus.
Vesico-urachal diverticulum is identified as a urine-filled anterosuperior extension from the bladder done on all imaging modalities.
A urachal diverticulum frequently coexists with congenital obstruction of the lower urinary tract. Rarely a malignancy can arise within the diverticulum: see urachal cancer.
Figure 4. Vesico-urachal diverticulum

Patent urachus
A patent urachus is one of the spectrum of congenital urachal anomalies. It has occasionally been termed “urachal fistula”. A patent urachus represents the failure of the entire course of the fetal allantois to involute into the median umbilical ligament. This results in an open channel between the bladder and the umbilicus.
A patent urachus is often diagnosed in neonates when urine is noted leaking from the umbilicus. The umbilicus may also have an abnormal appearance on physical exam.
If the patent urachus is very narrow, it may present later in life if high pressures in the bladder develop (e.g. bladder outlet obstruction), forcing urine through the patent urachus.
A patent urachus predisposes to infection.
Recommended treatment of a patent urachus is surgical excision, which has an excellent prognosis.
Patent urachus signs and symptoms
Patent urachus typically presents as persistent drainage or inflammation at the umbilicus in the newborn period. An anterior, midline cystic structure extending from the bladder dome to the anterior abdominal wall is diagnostic.
Visible signs
In newborns and infants, drainage or “wetness” of the belly button that does not go away can be a sign of a problem. The most common problem at the belly button is a granuloma. This is an area that is reddened because the base of the umbilical cord stump did not heal correctly.
Sometimes the area can be very red even after the umbilical cord stump comes off. Dabbing a small amount of alcohol on the site twice a day will often lead to full healing in 2 to 3 days. If the redness does not go away or gets worse, talk to your health care provider.
Other Signs
There can also be urachal issues without wetness. About 35% of these problems are from an enclosed or infected urachal cyst. This type of problem is seen more often in older children and adults. Instead of visible belly button drainage, the signs are:
- Lower belly pain
- Fever
- A lump that can be felt
- Pain with voiding (urinating)
- UTI (urinary tract infection)
- Blood in the urine (Hematuria)
Other health issues around the belly button
There have been a few reports of other problems causing pain and swelling with the umbilical cord. These include infections of the remnant blood vessels. Also, the vitelline duct, between the belly button and the small intestine, sometimes has its own remnant problems. Sometimes a health problem like appendicitis or an ovarian cyst can mimic some of the signs of urachal problems.
Patent urachus diagnosis
The most common test used to diagnosis urachal anomalies is an ultrasound of the abdomen, bladder and pelvis.
Figure 5. Patent urachus ultrasound

Footnote: 6 week old boy with umbilical granuloma treated with silver nitrate presents with continuous ongoing discharge from umbilicus. Anechoic tubular structure measuring 3 mm in width connects the anterior superior aspect of the urinary bladder to the anterior abdominal wall on longitudinal view. On transverse view, defect is visualized extending through the umbilicus.
[Source 2 ]Voiding Cystourethrogram
Sometimes a voiding cystourethrogram (an x-ray using contrast dye) is useful even after a physical exam and ultrasound. This is done when the draining urachus is linked to bladder outlet obstruction, which would also need to be treated. This is most often settled by the patient’s age, gender and physical exam.
Cystoscopy
In some cases a direct look into the bladder with a cystoscopy can be helpful. But most urologists suggest using the methods previously mentioned.
Persistent urachus treatment
Most urachal problems can be found with a physical exam and ultrasound.
Chemical cauterization for umbilical granuloma
This is done in the office of your primary care provider. An umbilical granuloma is a superficial abdominal wall problem. It will heal after treatment with antibiotics. There are usually no long-term issues.
Patent urachus – if there is a sinus (abnormal opening)
Unlike the simple granuloma, umbilical wetness that does not go away should be looked at by a urologist.
About 65% of all urachal problems appear as a sinus or drainage opening at the belly button. Most of those are not connected all the way to the bladder. But a few cases have an open pathway from the bladder to the belly button. This is called a patent urachus. This can be confirmed by testing urea and creatinine levels in the fluid. These levels would be high if the fluid was urine from a bladder connection.
Antibiotics for Infection
Redness can be caused by this drainage, as well as infection of the skin. If there is pain or fever, or the redness spreads to nearby skin, you will need prompt antibiotic treatment and a possible hospital stay. This type of infection of the umbilical stump is called omphalitis. It can be from bacteria from a urachal sinus. Or it could be caused by something else in the belly button area that once joined to the bowels.
Sinogram
Once the swelling is controlled, the opening at the belly button can be looked at with a sinogram. A small tube is placed into the sinus opening and contrast dye flows in. X-rays are then taken to look at the channel. If the channel follows the path to the top of the bladder, the diagnosis is urachal sinus.
Surgery
The urachus and all of its connections (plus a small amount of the top of the bladder) should be fully removed with surgery. Leaving any tissue behind could allow cancer to develop. Less than 1% of all bladder cancer occurs in the urachus. But once the urachus has potentially become a problem, it should be removed.
Urachus cyst – if there is no sinus
Imaging
When there is no draining sinus to look into, ultrasound of the lower belly will often show a fluid-filled, enclosed lump in the location of the urachus. In an adult with a small chance of cancer, abdominal and pelvic CT scans may also be helpful.
Antibiotics for Infected Cysts
About 80% of infected cysts contain Staphylococcus aureus and many other types of bacteria. An infected cyst almost always stays in the same place. Rarely, an infected cyst will drain into the space between the stomach and other organs, causing inflammation and fever. Antibiotics will heal the infection.
Surgery
Again, complete removal of the urachus is important. After simple drainage with a needle, urachal abnormalities come back in about a third of patients. This is because the linings and structures are still present.
After complete surgical removal of the urachus, there should be no further issues. There is no need for routine follow-up. But, you should reach out to your health care provider if you notice any changes.
Urachal cancer
A growth of cancerous cells that starts in the urachus is called urachal cancer. Urachal cancer is usually an adenocarcinoma (cancer from gland cells), but other forms of cancer can also occur. Because of its location, urachal cancer can grow into the abdominal wall and the abdominal cavity. Often it infiltrates the roof of the urinary bladder. Urachal cancer can grow for a long time before causing symptoms. As a result, it is often detected at later stages.
It is estimated that about 1 new case urachal cancer per year per 1 million people occurs. It seems as if there are variations in different regions of the world. Men are affected more often than women (about 60% are men) and urachal cancer is most often detected in the the 5th decade of life.
About 20% of urachal cancer patients cannot be cured by the time they develop symptoms. After treatment, about one-third will have relapse or their disease will spread. Average survival is 50% at 5 years.
What are the symptoms of urachal cancer?
In most cases, the first symptom is blood in the urine (haematuria). However, in 90% haematuria has benign reasonons, as for example bladder stones or infections. More uncommon symptoms in urachal cancer such us mucus discharge from the bladder (mucusuria) or umbilicus, local pain and recurrent bladder infections can occur. If possible, you can seek an urologist for further help with these symtpoms.
Urachal cancer diagnosis
This usually done by physical examination by your doctor and imaging techniques such as ultrasound, CT and cystoscopy. If rarely a tumour can be detected, usually a multidisciplinary team is involved in the diagnosis and further treatment.
Urachal cancer treatment
In early stages of the disease, surgical excision of the tumor can often cure the disease. This often is done by partial excision of the tumor containing bladder dome and tissue in the midline with the umbilicus.
In later stages and when urachal cancer has spread to other organs or sites, palliative chemotherapy can be an option. Regmies containing 5-Fluorouracil (5-FU) have been shown to be effective. In recent years also targeted therapy agents (for example cetuximab) known especially from cancer of the large bowel have also shown efficacy in some cases.
References- Bannon A, Black P, Turner J, Gray S, Kirk S. Belly button piercings: a saving grace? A patent urachus presenting in a 17-year-old girl. BMJ Case Rep. 2014;2014:bcr2014204336. Published 2014 Jun 10. doi:10.1136/bcr-2014-204336 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4054511
- Patent urachus ultrasound. https://radiopaedia.org/cases/patent-urachus-ultrasound





{kind=link}