What is angiotensin
Angiotensin is a peptide endocrine hormone and an important part of the renin-angiotensin-aldosterone system, an inter-related endocrine system important in blood volume and blood pressure control 1. Angiotensinogen, an alpha-globulin, and the peptide prohormone is synthesized primarily by the liver and circulates in plasma. When blood pressure drops, or when sympathetic signals reach the kidney, renin, a peptide produced primarily by the renal juxtaglomerular cells, is released and enzymatically cleaves off two amino acids forming angiotensin 1, a decapeptide. Angiotensin 1 is further cleaved into an octapeptide, angiotensin 2 by the action of angiotensin converting enzyme (ACE), primarily in the pulmonary endothelium, though this enzyme is present in the endothelium of other organs including the heart 1. Angiotensin 2 causes direct vasoconstriction of precapillary arterioles and postcapillary venules, inhibits the reuptake of norepinephrine, stimulates the release of catecholamines from the adrenal medulla, reduces urinary excretion of sodium and water, stimulates synthesis and release of aldosterone, and stimulates hypertrophy of both vascular smooth muscle cells and cardiac myocytes 2.
To block vasoconstriction and treat high blood pressure (hypertension) due to the effect of angiotensin 2, patients are often treated with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (ARBs) resulting in widening of your blood vessels. This reduces the pressure in the vessels and allows blood to flow more easily — making it easier for your heart to pump blood around your body. Angiotensin also stimulates the release of aldosterone from the adrenal cortex to promote sodium retention by the kidneys.
Angiotensin 2 has recently been given FDA approval for use in patients in shock 1. Angiotensin 2 is the active hormone and acts at angiotensin 2 receptors. Animal studies suggested that angiotensin 2 was safe and effective in increasing blood pressure in shock. Furthermore, after a small human trial showed success, the direct use of angiotensin 2 as a vasopressor (powerful class of drug that causes vasoconstriction and thereby elevate mean arterial pressure) was studied on critically ill patients. The results of the ATHOS-3 trial results were published in the August 2017 New England Journal of Medicine 3. The drug was studied in a placebo-controlled, double-blinded protocol with 321 subjects in the intensive care unit setting. Multiple hospitals in nine countries recruited severely ill patients with septic and vasodilatory shock who were not adequately responding to fluid and high-dose norepinephrine or equivalent standard of care vasopressors. Treatment with synthetic human angiotensin 2 resulted in statistically significant improvements in mean arterial pressure in the treatment group. The primary endpoints included achieving mean arterial pressure greater than or equal to 75 mm Hg in the first 3 hours of infusion, and blood pressure maintenance with decreased use of vasopressors including epinephrine, norepinephrine, and dopamine at 48 hours. While the originally published analysis of the data did not show a statistically significant mortality benefit, additional analysis has shown a statistically significant reduction in mortality at 28 days in a subgroup of treated patients.
In December of 2017, after a priority review, intravenous (IV) synthetic human angiotensin 2 was approved by the FDA for the treatment of septic and other distributive, vasodilatory shock in adults 4.
Clinical trials for the use of angiotensin 2 in pediatric patients with refractory shock are currently recruiting patients.
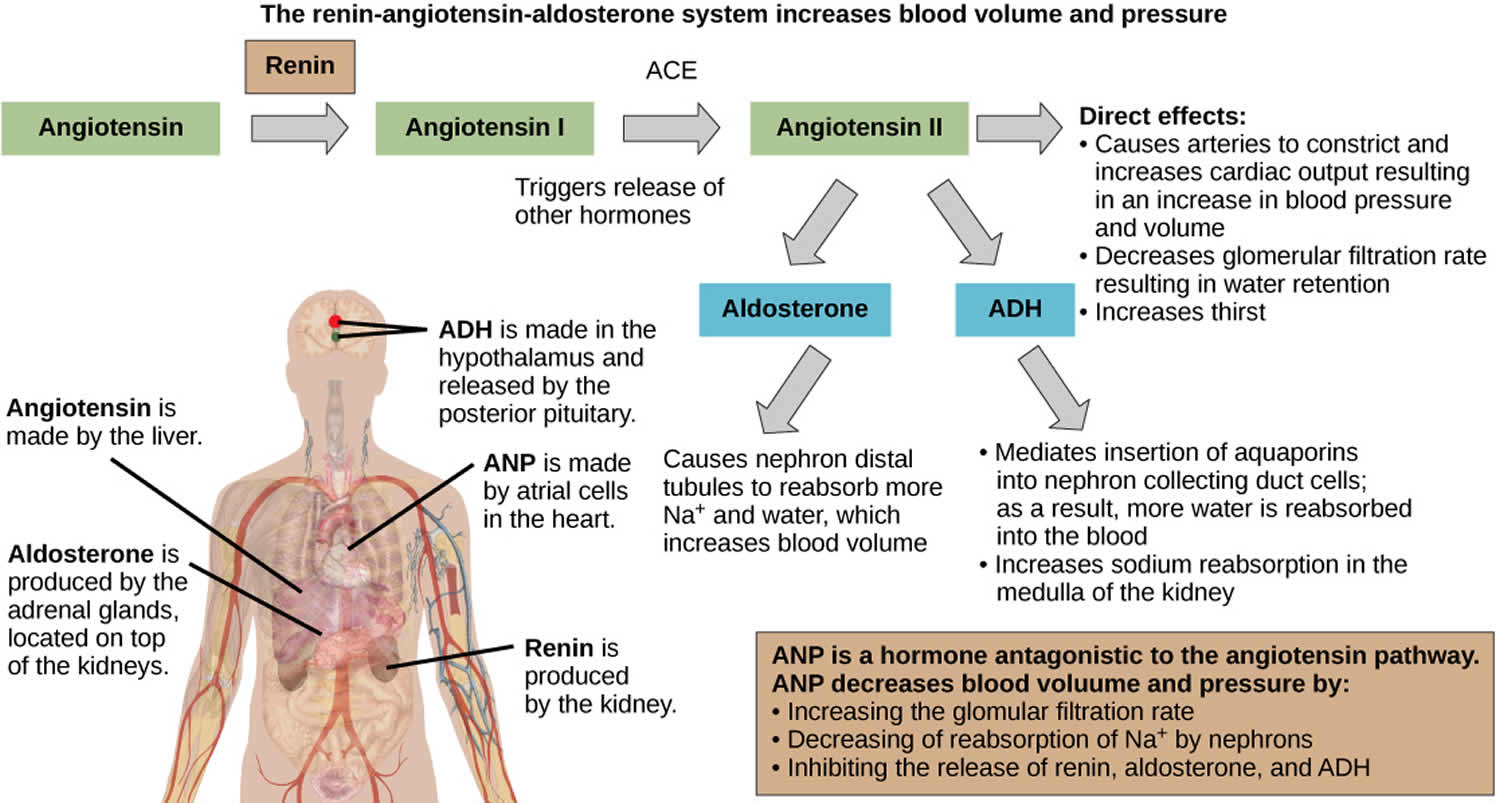
Figure 1. Renin angiotensin aldosterone system
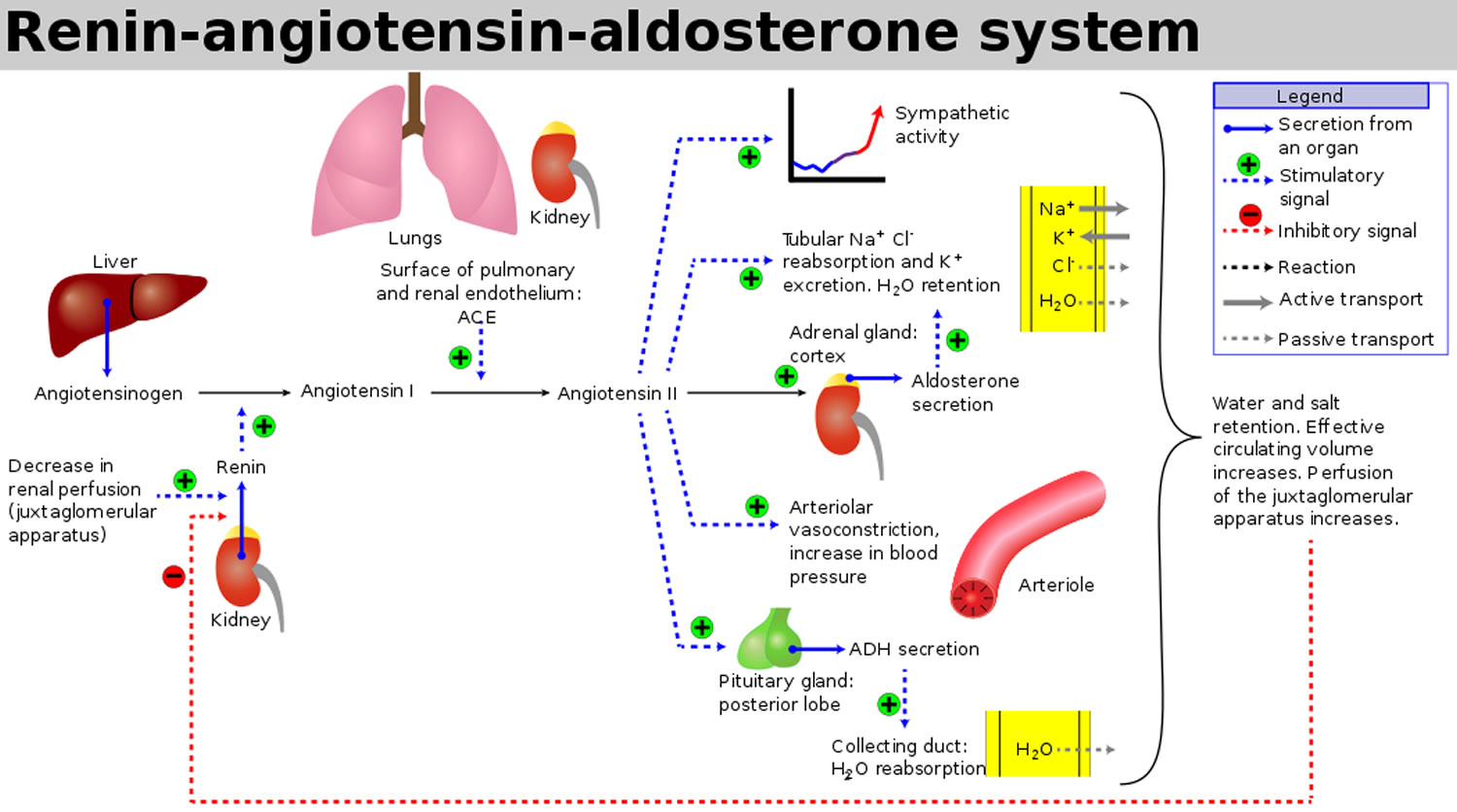
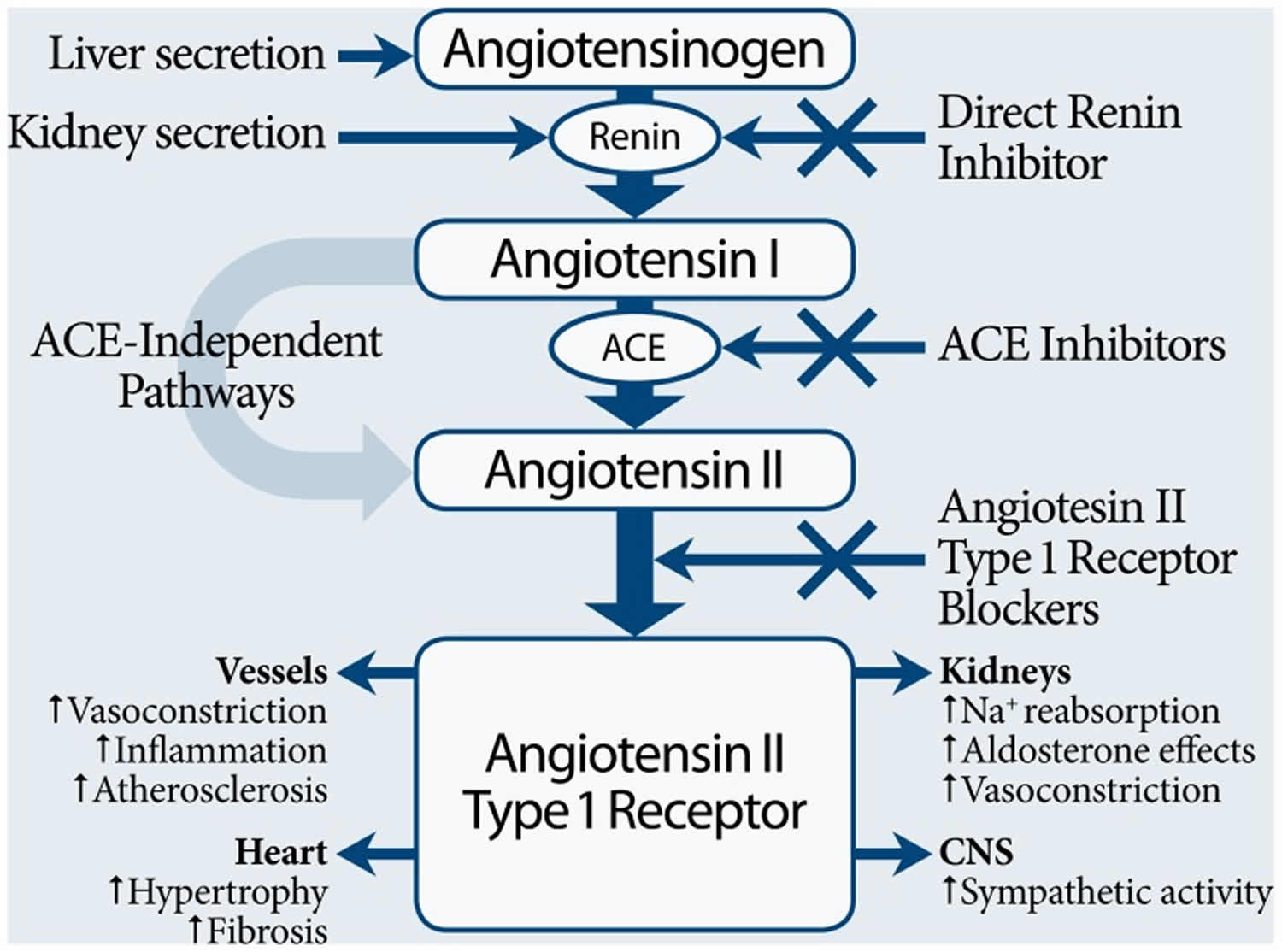
Figure 2. Angiotensin 1 and Angiotensin 2 production
What does angiotensin 2 do?
Angiotensin 2 is a potent vasopressor, acting on vascular endothelial receptors. The two types of angiotensin 2 receptors present in the heart and vasculature smooth muscle that are responsible for signal transduction in mediating the vasoconstrictive action of angiotensin 2 are the angiotensin 1 and angiotensin 2 receptors 6. Their signaling leads to calcium-dependent phosphorylation of myosin which leads to contraction of the vascular smooth muscle. This arterial smooth muscle contraction is responsible for raising blood pressure.
In addition, angiotensin 2 interacts with angiotensin receptors at various sites in the nephron to stimulate sodium reabsorption. Angiotensin 2 also acts on the zona glomerulosa of the adrenal cortex to stimulate the release of aldosterone, a steroid hormone that acts in the kidney to promote sodium and water retention.
Angiotensin-converting enzyme inhibitors (ACEI) may increase the effect of intravenous angiotensin 2, and the use of angiotensin receptor blockers (ARBs) may reduce the effect of intravenous angiotensin 2. The mechanism for the interaction with angiotensin-converting enzyme inhibitors (ACEI) is not specified. The interaction with angiotensin receptor blockers (ARB) is by pharmacodynamic antagonism of the drug at the receptor site.
Angiotensin 2 is not only involved in the regulation of blood pressure, water and sodium homeostasis, and control of other neurohumoral systems, but also leads to excessive production of reactive oxygen species (ROS) and to hypertrophy, proliferation, migration, and apoptosis of vascular cells 7. Angiotensin 2 is one of the main factors involved in hypertension-induced tissue damage 8. Angiotensin 2 regulates the inflammatory process 9. Angiotensin 2 activates circulating cells, and participates in their adhesion to the activated endothelium and subsequent transmigration through the synthesis of adhesion molecules, chemokines and cytokines. Among the intracellular signals involved in angiotensin 2-induced inflammation, the production of reactive oxygen species and the activation of nuclear factor-kappaB are the best known 9. Classical, well-defined actions of angiotensin 2 in the brain include the regulation of hormone formation and release, the control of the central and peripheral sympathoadrenal systems, and the regulation of water and sodium intake. As a consequence of changes in the hormone, sympathetic and electrolyte systems, feedback mechanisms in turn modulate the activity of the brain angiotensin 2 systems. There are two angiotensin 2 systems in the brain 10. The discovery of brain angiotensin 2 receptors located in neurons inside the blood brain barrier confirmed the existence of an endogenous brain angiotensin 2 system, responding to angiotensin 2 generated in and/or transported into the brain. In addition, angiotensin 2 receptors in circumventricular organs and in cerebrovascular endothelial cells respond to circulating angiotensin 2 of peripheral origin. Thus, the brain responds to both circulating and tissue angiotensin 2, and the two systems are integrated 10.
Angiotensin 2 medication
Angiotensin 2 is only available in an intravenous form for IV administration through a central venous line 1. Angiotensin 2 drug is available in vials of 2.5 mg/mL and 5 mg/2mL. One vial of the drug is diluted in 0.9% sodium chloride solution to a concentration of either 5000 ng/mL or 10,000 ng/mL prior to infusion 1. The higher concentration is used in patients who are fluid restricted.
It is started at an infusion of 20 ng/kg per minute and titrated up as needed to a maximum dose of 80 ng/kg per minute during the first 3 hours of use and a maximum maintenance dose of 40 ng/kg/min 1.
Monitoring
Patients on angiotensin 2 drug are treated in an intensive care setting with concomitant intensive hemodynamic monitoring, including mean arterial pressure. Blood pressure monitoring is especially important since hypertension is a potential direct adverse effect of the drug. Angiotensin 2 has a plasma half-life of less than a minute, so with careful monitoring, hypertension can be quickly reversed.
The angiotensin 2 drug should be carefully titrated based on blood pressure response to a mean arterial pressure of 75 or greater.
Because of the potential for both arterial and venous thromboembolic events, all treated patients should receive concurrent deep vein thrombosis (DVT) prophylaxis.
Because of the effects of angiotensin 2 on the kidneys and other parts of the renin-angiotensin-aldosterone system, it is prudent to monitor kidney function with BUN (blood urea nitrogen) and serum creatinine. Serum potassium should be monitored as well. The potential for thrombocytopenia suggests monitoring of complete blood count (CBC) including platelet counts.
Angiotensin 2 side effects
Most common side effects during angiotensin 2 clinical trials 3:
- Thromboembolic events (12.9%) including DVT (4.3%)
- Thrombocytopenia (9.8%)
- Tachycardia (8.6%)
Other adverse reactions occurring at greater than 4%:
- Fungal infection
- Delirium
- Acidosis
- Hyperglycemia
- Peripheral ischemia
Safety of the active drug was similar to placebo. Compared with placebo, fewer patients receiving angiotensin 2 required discontinuation of the drug due to serious adverse events. The rates of anticipated adverse events such as tachyarrhythmias, ventricular tachycardia, atrial tachycardia, and distal ischemia were similar between the two groups.
Angiotensin 2 contraindications
No contraindications are included in the prescribing information. Nearly half of the study population was over 65, and safety data was no different for patients under versus over that age. No data exists for the use of angiotensin 2 in pediatric patients at this time, though clinical trials have begun. The potential for mutagenicity, carcinogenicity, or adverse effects on fertility have not been studied.
Toxicity
The pharmacologic effect of angiotensin 2 drug is to raise blood pressure. An overdose of the angiotensin 2 drug could result in hypertension. Careful monitoring and titration of the angiotensin 2 drug should prevent this effect, but the short plasma half-life of angiotensin 2 means that this toxicity can be easily reversed and no antidote or further treatment should be required. The potential for thromboembolic events in patients treated with angiotensin II dictates the need for DVT prophylaxis during treatment.
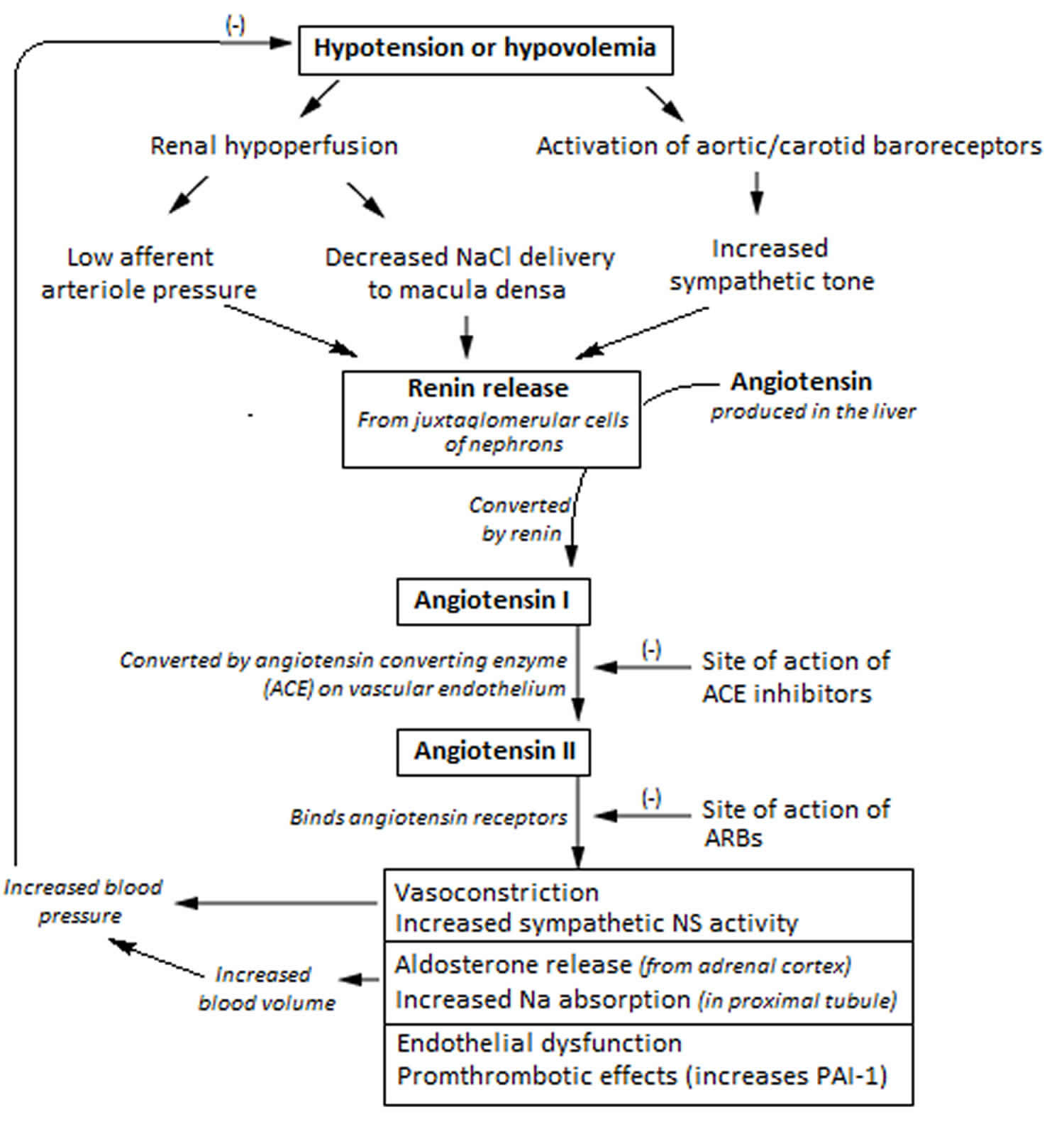
Renin angiotensin aldosterone system
The renin–angiotensin–aldosterone system (RAAS) is a critical regulator of blood volume and systemic vascular resistance. The renin–angiotensin–aldosterone system functions to elevate blood volume and arterial tone in a prolonged manner. The renin–angiotensin–aldosterone system does this by increasing sodium reabsorption, water reabsorption, and vascular tone. While the baroreceptor reflex responds in a short-term manner to decreased arterial pressure, the renin angiotensin aldosterone system is responsible for more chronic alterations 11. The renin–angiotensin–aldosterone system (RAAS) is composed of three major compounds: renin, angiotensin 2 and aldosterone. These three act to elevate arterial blood pressure in response to decreased renal blood pressure, decreased salt delivery to the distal convoluted tubule, and/or beta-agonism. Through these mechanisms, the body can elevate the blood pressure in a prolonged manner.
The renin angiotensin aldosterone system acts to manage blood volume and arteriolar tone on a long-term basis. While minor and rapid shifts are typically managed via the baroreceptor reflex, the renin angiotensin aldosterone system can alter blood volume chronically. Though the renin angiotensin aldosterone system serves a critical function, it can be activated inappropriately in several conditions that may then lead to the development of hypertension. For example, renal artery stenosis results in a decreased volume of blood reaching one (or both) kidneys. As a result, the juxtaglomerular cells will sense a decrease in blood volume, activating the renin angiotensin aldosterone system. This can lead to an inappropriate elevation of circulating blood volume and arteriolar tone due to poor renal perfusion.
Pharmacologically, the renin angiotensin aldosterone system (RAAS) is a frequently manipulated system in the management of heart failure, hypertension, diabetes mellitus, and acute myocardial infarction. Angiotensin converting enzyme inhibitors (e.g., enalapril), angiotensin receptor blockers (ARBs, e.g., losartan), and aldosterone antagonists (e.g., spironolactone) all act to decrease the effect of the renin angiotensin aldosterone system.
The varied mechanisms of these drugs allow their utilization in different scenarios. Angiotensin converting enzyme inhibitors inhibit the action of angiotensin-converting enzymes, thus decreasing the production of angiotensin 2. Angiotensin receptor blockers (ARBs) act to block angiotensin receptors, thus inhibiting angiotensin’s effect while maintaining normal levels of the compound. Aldosterone inhibitors have two specific varieties. The first (e.g., spironolactone or eplerenone) act as aldosterone antagonists. These work by preventing the binding of aldosterone to binding sites in the kidney, preventing insertion of Na channels. The second (e.g., amiloride or triamterene) group act to block the inserted Na (sodium) channels in the distal convoluted tubule.
A common use for angiotensin converting enzyme inhibitors or angiotensin receptor blockers (ARBs) is in the management of hypertension. In these cases, blocking or decreasing levels of angiotensin 2 will lead to a reduction in blood pressure. They achieve this goal by decreasing sodium and water reabsorption, leading to a reduction in blood volume, and decreasing arteriolar tone. In addition, these drugs are often used in the management of diabetes mellitus. Patients with diabetes mellitus often have renal manifestations such as proteinuria due to excess glucose damaging the glomerulus. Using angiotensin converting enzyme inhibitors or angiotensin receptor blockers (ARBs) can decrease efferent arteriolar tone, leading to a reduction in pressure on the glomerulus. Thus, they are frequently used for prevention of worsening diabetic nephropathy.
Figure 3. The renin angiotensin aldosterone system involves the kidneys, lungs, systemic vasculature, and the brain.
Renin angiotensin aldosterone system mechanism of action
Within the afferent arterioles of the kidney, specialized cells called juxtaglomerular cells contain prorenin. While prorenin is secreted constitutively in its inactive form, activation of juxtaglomerular cells causes the cleavage of prorenin to renin. Activation of these cells occurs in response to decreased blood pressure, beta-activation, or activation by macula densa cells in response to a decreased sodium load in the distal convoluted tubule.
Once renin has been released into the blood, it can act on its target, angiotensinogen. Angiotensinogen is produced in the liver and is found continuously circulating in the plasma. Renin then acts to cleave angiotensinogen into angiotensin 1. Angiotensin 1 is physiologically inactive, but acts as a precursor for angiotensin 2.
The conversion of angiotensin 1 to angiotensin 2 is catalyzed by an enzyme called angiotensin converting enzyme (ACE). Angiotensin converting enzyme (ACE) is found primarily in the vascular endothelium of the lungs and kidneys. After angiotensin 1 is converted to angiotensin 2, it has effects on the kidney, adrenal cortex, arterioles, and brain by binding to angiotensin 2 type I and type II receptors. The effects discussed below are a result of binding to angiotensin receptors. The role of angiotensin receptors is still being investigated, but pertinently, they have been shown to cause vasodilation by nitric oxide generation. In the plasma, angiotensin 2 has a half-life of 1-2 minutes, at which point peptidases degrade it into angiotensin 3 and 4. Angiotensin 3 has been shown to have 100% of the aldosterone stimulating effect of angiotensin 2, but 40% of the pressor effects, while angiotensin 4 has some lesser pressor effect 11. Angiotensin 4 has cognitive-enhancing effects in the central nervous system 12. The exact identity of angiotensin 4 receptors has not been established. There is evidence that the angiotensin 4 receptor is insulin-regulated aminopeptidase 13 receptor is the enzyme insulin-regulated aminopeptidase. J Biol Chem. 2001 Dec 28;276(52):48623-6. Epub 2001 Nov 13. http://www.jbc.org/content/276/52/48623.long)). There is also evidence that angiotensin 4 interacts with the hepatocyte growth factor (HGF) through the c-Met receptor 14.
Synthetic small molecule analogues of angiotensin 4 with the ability to penetrate through blood brain barrier have been developed 15.
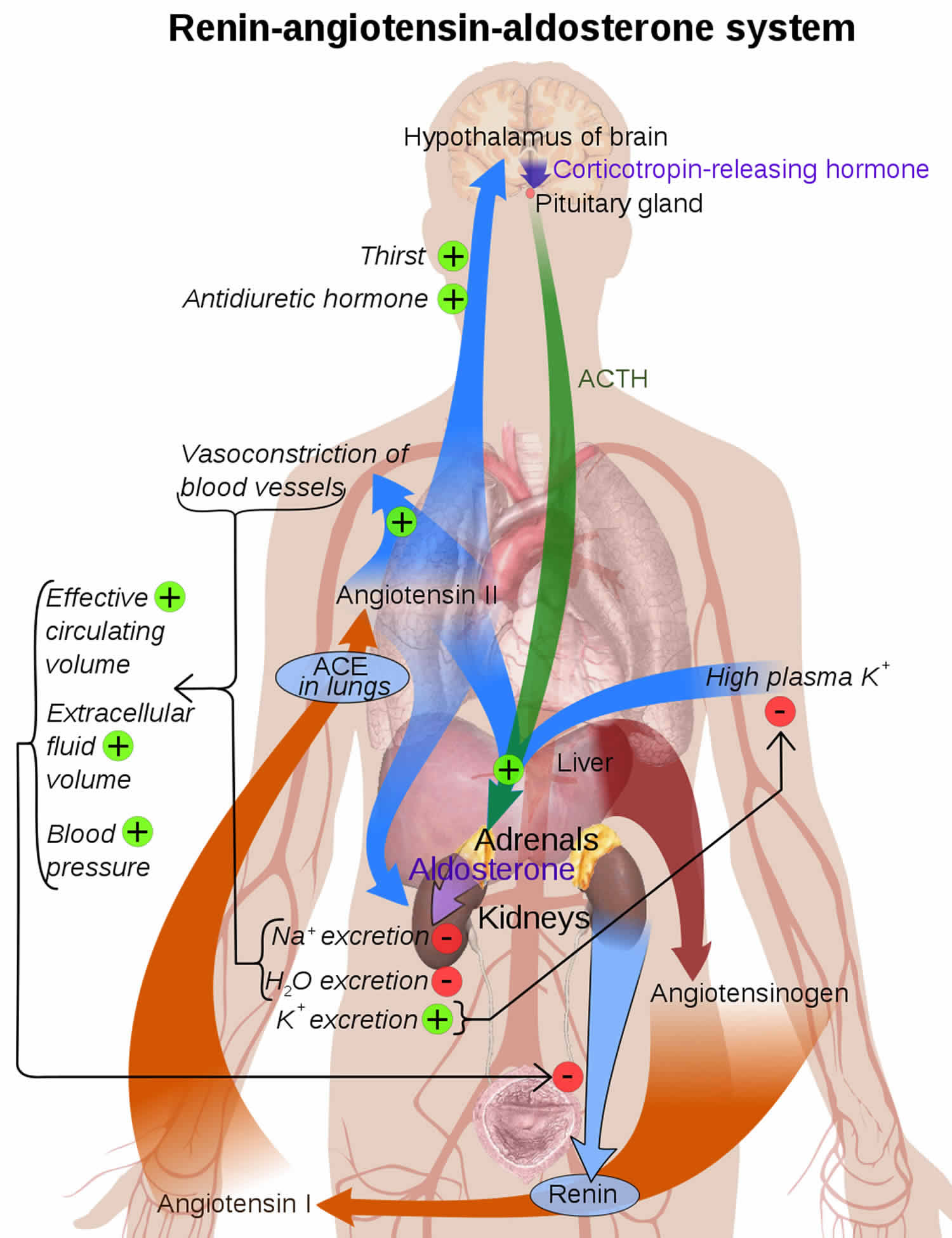
Figure 4. Renin angiotensin aldosterone system mechanism of action
 In the proximal convoluted tubule of the kidney, angiotensin 2 acts to increase Na-H exchange, increasing sodium reabsorption. Increased levels of Na in the body acts to increase the osmolarity of the blood, leading to a shift of fluid into the blood volume and extracellular space (ECF). This increases the arterial pressure of the patient.
In the proximal convoluted tubule of the kidney, angiotensin 2 acts to increase Na-H exchange, increasing sodium reabsorption. Increased levels of Na in the body acts to increase the osmolarity of the blood, leading to a shift of fluid into the blood volume and extracellular space (ECF). This increases the arterial pressure of the patient.Angiotensin 2 also acts on the adrenal cortex, specifically the zona glomerulosa. Here, it stimulates the release of aldosterone. Aldosterone is a steroid hormone that causes an increase in sodium reabsorption and potassium excretion at the distal tubule and collecting duct of the nephron. Aldosterone works by stimulating the insertion of luminal Na channels and basolateral Na-K ATPase proteins. The net effect is an increased level of sodium reabsorption. This has the same effect as mentioned previously: the increased total body sodium leads to an increase in osmolarity and subsequent increase in blood and extracellular space (ECF) volume. In contrast to angiotensin II, aldosterone is a steroid hormone. As a result, it enacts change by binding to nuclear receptors and altering gene transcription. Thus, the effects of aldosterone may take hours to days to begin, while the effects of angiotensin 2 are rapid.
The effect of angiotensin II on vasoconstriction takes place in systemic arterioles. Here, angiotensin 2 binds to G protein-coupled receptors, leading to a secondary messenger cascade that results in potent arteriolar vasoconstriction. This acts to increase total peripheral resistance, causing an increase in blood pressure.
Finally, angiotensin 2 acts on the brain. Here, it has three effects. First, it binds to the hypothalamus, stimulating thirst and increased water intake. Second, it stimulates the release of antidiuretic hormone (ADH) by the posterior pituitary. Antidiuretic hormone (ADH), or vasopressin, acts to increase water reabsorption in the kidney by inserting aquaporin channels at the collecting duct. Finally, angiotensin 2 decreases the sensitivity of the baroreceptor reflex. This diminishes baroreceptor response to an increase in blood pressure, which would be counterproductive to the goal of the renin angiotensin aldosterone system.
The net effect of these interactions is an increase in total body sodium, total body water, and vascular tone.
Angiotensin converting enzyme inhibitors
In 2014, the Eighth Joint National Commission 16 published evidence-based guidelines for the treatment of high blood pressure in adults which recommended that angiotensin-converting enzyme inhibitors are one of four drug classes recommended for initial therapy for adults with elevated blood pressure. The other three classes of drugs are calcium channel blockers, thiazide diuretics, and angiotensin receptor blockers (ARBs) which can be used as initial therapy for the general nonblack population. Only thiazide and calcium channel blockers are recommended as initial therapy for the general black population with elevated blood pressure 16.
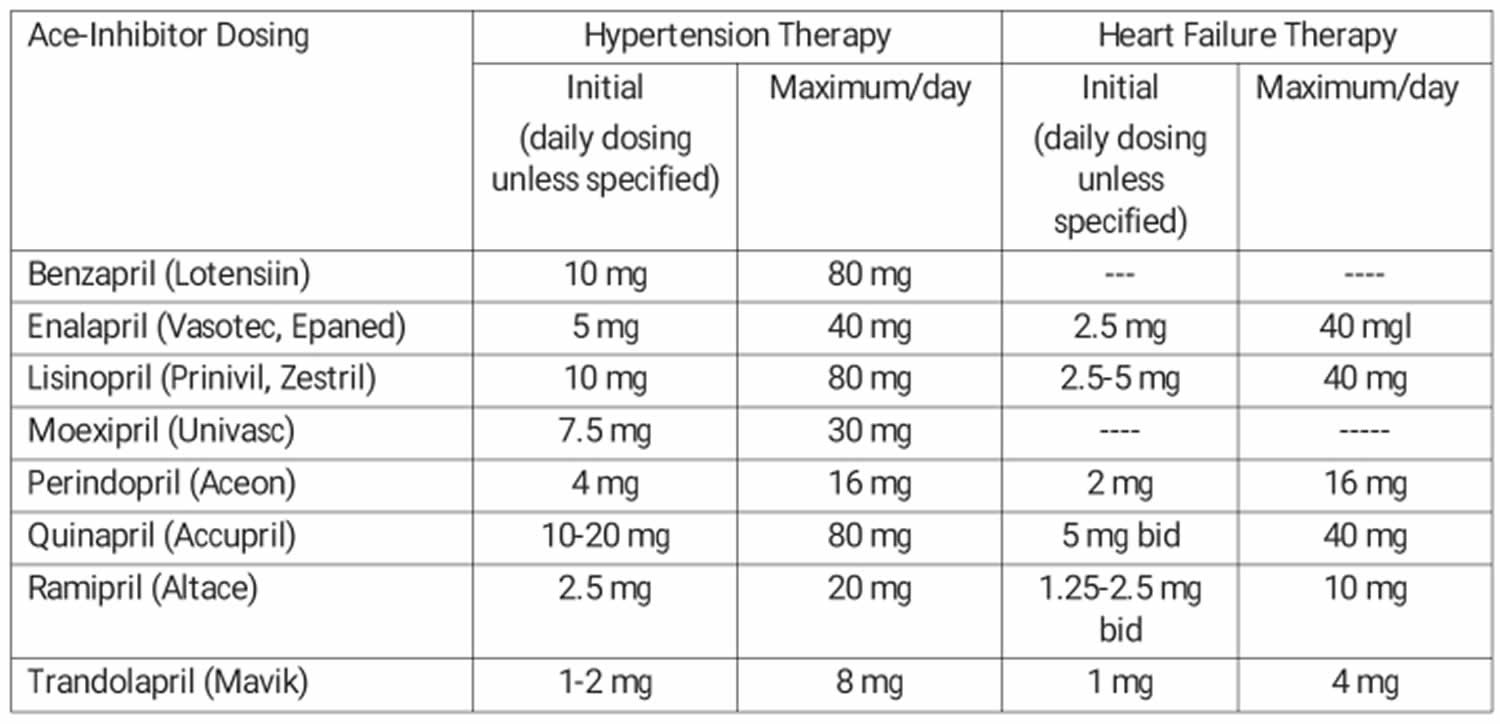
Table 1. Angiotensin-converting enzyme inhibitors
Heart Failure
It is the decrease in afterload which improves heart failure. Also, those with heart failure have less myocyte hypertrophy when angiotensin-converting enzyme inhibitors are used. Also, the Heart outcomes Prevention Evaluation Study 17 demonstrated better outcomes for those that were prescribed angiotensin-converting enzyme inhibitors.
Asymptomatic Left Ventricular Dysfunction
Angiotensin-converting enzyme inhibitors have been shown to decrease the incidence of overt heart failure.
Post Myocardial Infarction
In 2000, The Heart Outcomes Prevention Evaluation Study 18 investigators published a landmark study demonstrating significantly reduced rates of death, myocardial infarction, and stroke in high-risk patients assigned to receive the angiotensin-converting enzyme inhibitor, ramipril.
Since the HOPE Study, several angiotensin converting enzyme inhibitors have been studied. Most of the patients in those studies had an ST-elevation myocardial infarction (heart attack). Most patients had not received a percutaneous coronary intervention (PCI, formerly known as angioplasty with stent) but had received fibrinolytic therapy or no reperfusion, so data on the benefit with the addition of angiotensin-converting enzyme inhibitors in patients receiving percutaneous coronary intervention (angioplasty with stent) is limited. The research continued to demonstrate decreased mortality for patients with low left ventricular ejection fraction, heart failure or anterior myocardial infarctions that are begun on angiotensin-converting enzyme inhibitors. Other positive effects have been decreasing in readmission for heart failure and decrease in the incidence of re-infarction.
It is suggested that the angiotensin-converting enzyme inhibitor be given with a diuretic.
Angiotensin-converting enzyme inhibitors dosage
Angiotensin-converting enzyme inhibitors available are grouped into three main groups depending on their chemical structure:
- Sulfhydryl-containing angiotensin-converting enzyme inhibitor of which there is only 1.
- Captopril (Capoten) – Hypertension therapy is 25 mg either twice daily or three times daily with a maximum of 450 mg.
- Heart Failure therapy is 6.25 mg three times daily with a maximum of 450 mg.
- Dicarboxylic-containing angiotensin-converting enzyme inhibitors: see Table 1
- Phosphorus-containing angiotensin-converting enzyme inhibitor of which there is only one.
- Fosinopril (Monopril) – Hypertension therapy dosing is 10 mg increasing to a maximum dose of 80 mg. May split into two equal doses during the day to control blood pressure. Heart failure therapy is 5 – 10 mg daily to a maximum dose of 40 mg.
General information about dosing:
All of the angiotensin-converting enzyme inhibitors are taken orally except for enalapril which can be given intravenously. The dosage is 1.25 mg every 6 hours. It can be increased to 5 mg every 6 hours.
The dosage should be decreased in patients with heart failure, salt-depleted patients, and/or renal impairment.
Lisinopril and captopril are the only angiotensin-converting enzyme inhibitors that do not have to be activated in the body to be effective. All the other angiotensin-converting enzyme inhibitors are prodrugs and require activation. Most reach peak serum levels within 1 hour after ingestion. Since most of the activation occurs in the liver, when a patient has a severe hepatic failure, a nonprodrug form should be used. The doses of the prodrugs can be increased though in those with some degree of poor hepatic function.
Monitoring
Renal function and electrolytes need to be checked on a regular basis due to the effects of the drug on the renin-angiotensin-aldosterone system. Those with increasing potassium, BUN (blood urea nitrogen) and creatinine need to have the drug discontinued.
Since angiotensin-converting enzyme inhibitors can have an affect upon the liver, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) should also be monitored.
Angiotensin-converting enzyme inhibitors side effects
About 1 -10% will develop a dry, nonproductive paroxysmal cough. The patient must then decide if they can tolerate a cough and continue the medication. There is no treatment for a cough.
Angioedema is the most significant. It can be of any part of the body including intestine, but the most concerning is edema of the tongue, glottis and/or larynx causing airway obstruction. There have been reported fatal cases. Angioedema has a higher rate of incidence in the Afro-American population. When airway compromise is present, the treatment is always securing the airway with an endotracheal tube that allows ventilation until the edema resolves. Multiple treatments have been tried such as diphenhydramine, methylprednisolone, and epinephrine. Also, fresh frozen plasma and the newer agents, bradykinin blocking agents have been tried. There are case reports that these bradykinin blocking agents might improve the angioedema but no literature exists proving that they are better than previous treatment. There is an on-going Phase III trial at this time.
Life-threatening anaphylactoid reactions have occurred in patients receiving Hymenoptera venom desensitization treatment and also in patients being dialyzed with high-flux membranes. Treatment includes diphenhydramine, epinephrine and blood pressure support with fluids and catecholamines.
These drugs have been known to cause renal failure. Those with heart failure who depend on the renin-angiotensin-aldosterone system may develop changes in renal function with the use of angiotensin-converting enzyme inhibitors. Also, about 1/5 of patients with renal artery stenosis develop increases in blood urea nitrogen and creatinine. Any patient who already has a renal insufficiency is susceptible to worsening of renal function. The renal function needs to be monitored during treatment for susceptible groups.
As with any medication that lowers blood pressure, hypotension is an adverse reaction. Those at risk for this side effect: heart failure with a systolic blood pressure below 100 mmHg, ischemic heart disease, cerebrovascular disease, hyponatremia, high dose diuretic therapy, renal dialysis, or severe volume and/or sodium depletion.
Angiotensin-converting enzyme inhibitors may cause hyperkalemia. Those at risk for this side effect: prior history of renal impairment and/or diabetes, simultaneous use of potassium-sparing diuretics and/or potassium supplements. Treatment depends upon the level of potassium, EKG changes, and whether the patient still has kidney function and produces urine.
There has been one report of increased sudden death in patients taking angiotensin-converting enzyme inhibitors and Co-trimoxazole simultaneously. The mechanism is believed to be hyperkalemia.
Cholestatic jaundice or hepatitis is another serious adverse affect which can progress to hepatic necrosis and sometimes death. The drug needs to be discontinued, and the patient managed in the appropriate way.
Angiotensin-converting enzyme inhibitors contraindications
They are contraindicated in patients with a history of angioedema or hypersensitivity related to treatment with an angiotensin-converting enzyme inhibitor and those with hereditary or idiopathic angioedema.
Should not be given to patients that are already taking a direct renin inhibitor such as aliskiren (tekturna).
Should not be given in pregnancy. It is a Category D in Pregnancy because it is known to cause skull hypoplasia, anuria, hypotension, renal failure, lung hypoplasia, skeletal deformations, oligohydramnios, and death.
Toxicity
Angiotensin-converting enzyme inhibitors overdoses are usually well tolerated, but significantly large dose can cause hypotension which is prolonged. Also, angiotensin-converting enzyme inhibitors block aldosterone which enhances potassium excretion of the body. When Aldosterone is blocked, potassium can accumulate, and sodium excretion is enhanced. Both lead to hyperkalemia and hyponatremia.
If the patient presents within 1 hour of ingestion and is awake and able to protect their airway, activated charcoal can be given. If they remain asymptomatic for 6 hours of observation, they can be considered medical stable for either discharge or referral to a mental health center depending on the circumstances of the overdose.
For those with hypotension, fluids should be the first line of therapy. There is no antidote for angiotensin-converting enzyme inhibitor poisoning. Naloxone has been used in captopril overdoses in the past with some success and can be tried if intravenous fluids are not successful. Also, vasopressors can be used for treatment of the hypotension.
Angiotensin converting enzyme test
Angiotensin converting enzyme (ACE) participates in the renin-angiotensin-aldosterone system in response to hypovolemia. Angiotensin converting enzyme (ACE) peptidase action on the decapeptide angiotensinogen 1 results in the hydrolysis of a terminal histidyl leucine dipeptide and the formation of the octapeptide angiotensin 2, a potent vasoconstrictor that increases blood pressure.
The primary source of angiotensin-converting enzyme is the endothelium of the lung. The angiotensin-converting enzyme (ACE) test is primarily ordered to help diagnose and monitor sarcoidosis. Sarcoidosis is a systemic disorder of unknown cause that often affects the lungs but may also affect many other body organs, including the eyes, skin, nerves, liver, and heart. Sarcoidosis is a disorder in which small nodules of immune and inflammatory cells and fibrous tissue that form nodules under the skin and in organs throughout the body called granulomas. Granulomas change the structure of the tissues around them and, in sufficient numbers, they can cause damage and inflammation and may interfere with normal functions. The cells found at the outside borders of granulomas can produce increased amounts of angiotensin-converting enzyme. The level of angiotensin-converting enzyme in the blood may increase when sarcoidosis-related granulomas develop. Angiotensin-converting enzyme (ACE) test is often ordered as part of an investigation into the cause of a group of troubling chronic symptoms that are possibly due to sarcoidosis. Serum angiotensin-converting enzyme is significantly higher in most (approximately 80%) patients with active sarcoidosis.
The blood level of angiotensin-converting enzyme tends to rise and fall with sarcoidosis disease activity. If angiotensin-converting enzyme is initially elevated in someone with sarcoidosis, the angiotensin-converting enzyme test can be used to monitor the course of the disease and the effectiveness of corticosteroid treatment.
A health practitioner may order angiotensin-converting enzyme along with other tests, such as AFB (Acid-Fast Bacillus) tests that detect mycobacterial infections or fungal tests. This may help to differentiate between sarcoidosis and another condition causing granuloma formation.
When is angiotensin-converting enzyme test ordered?
Angiotensin converting enzyme activity is increased in sarcoidosis, a systemic granulomatous disease that commonly affects the lungs. In sarcoidosis, angiotensin converting enzyme is thought to be produced by epithelioid cells and macrophages of the granuloma.
An angiotensin-converting enzyme test is ordered when someone has signs or symptoms that may be due to sarcoidosis, such as:
- Granulomas
- A chronic cough or shortness of breath
- Red, watery eyes
- Joint pain
This is especially true if the person is between 20 and 40 years of age, when sarcoidosis is most frequently seen.
When someone has been diagnosed with sarcoidosis and initial angiotensin-converting enzyme levels were elevated, a health practitioner may order angiotensin-converting enzyme testing at regular intervals to monitor the change in angiotensin-converting enzyme over time as a reflection of disease activity.
What does the angiotensin-converting enzyme test result mean?
An increased angiotensin-converting enzyme level in a person who has clinical findings consistent with sarcoidosis means that it is likely that the person has an active case of sarcoidosis, if other diseases have been ruled out. Angiotensin-converting enzyme will be elevated in 50% to 80% of those with active sarcoidosis. The finding of a high angiotensin-converting enzyme level helps to confirm the diagnosis.
Note: Angiotensin-converting enzyme inhibitors are useful in managing hypertension, but they interfere with angiotensin-converting enzyme measurements ordered for other reasons.
Currently, it appears that angiotensin-converting enzyme activity reflects the severity of sarcoidosis:
- 68% positivity in those with stage 1 sarcoidosis,
- 86% in stage 2 sarcoidosis, and
- 91% in stage 3 sarcoidosis.
An elevation in the level of serum angiotensin converting enzyme (ACE), along with radiographic evidence of infiltrates or adenopathy and organ biopsies showing noncaseating epithelial granulomas is suggestive of a diagnosis of sarcoidosis.
Serum angiotensin-converting enzyme also appears to reflect the activity of sarcoidosis disease. When monitoring the course of sarcoidosis disease, an angiotensin-converting enzyme level that is initially high and then decreases over time usually indicates spontaneous or therapy-induced remission and a favorable prognosis. For example, there is a dramatic decrease in enzyme activity in some patients receiving prednisone. A rising level of angiotensin-converting enzyme, on the other hand, may indicate either an early sarcoidosis disease process that is progressing or sarcoidosis disease activity that is not responding to therapy.
- Other conditions such as Gaucher disease, leprosy, untreated hyperthyroidism, psoriasis, premature infants with respiratory distress syndrome, adults with amyloidosis, and histoplasmosis have been associated with increased levels of angiotensin-converting enzyme.
- And in approximately 5% of the normal adult population serum angiotensin-converting enzyme is elevated.
A normal angiotensin-converting enzyme level cannot be used to rule out sarcoidosis because sarcoidosis can be present without an elevated angiotensin-converting enzyme level. Findings of normal angiotensin-converting enzyme levels in sarcoidosis may occur if the disease is in an inactive state, may reflect early detection of sarcoidosis, or may be a case where the cells do not produce increased amounts of angiotensin-converting enzyme. angiotensin-converting enzyme levels are also less likely to be elevated in cases of chronic sarcoidosis.
High and low levels of angiotensin-converting enzyme may be seen in a variety of conditions other than sarcoidosis. The angiotensin-converting enzyme test, however, is not routinely used to diagnose or monitor these conditions; it has not been shown to be clinically useful.
Decreased angiotensin-converting enzyme levels may also be seen in people with:
- Chronic obstructive pulmonary disease (COPD)
- Lung diseases such as emphysema, lung cancer, cystic fibrosis
- Starvation
- Steroid drug therapy
- Hypothyroidism
Angiotensin-converting enzyme has been found in moderately increased levels in a variety of diseases and disorders, such as:
- HIV
- Histoplasmosis (fungal respiratory infection)
- Diabetes mellitus
- Hyperthyroidism
- Lymphoma
- Alcoholic cirrhosis
- Gaucher disease (a rare inherited lipid metabolism disorder)
- Tuberculosis
- Leprosy
What causes sarcoidosis?
The cause of sarcoidosis is not well understood. Sarcoidosis is not contagious. Sarcoidosis is inflammatory and involves the immune system. It appears to have a genetic component as well as an environmental one. Sarcoidosis has been reported both in related and unrelated individuals living in the same area. Up to 40 people per 100,000 are affected in the U.S., the majority of them between 20 and 40 years old. In the U.S. and in the Caribbean, sarcoidosis is more common in those of African descent, but worldwide about 80% of those with sarcoidosis are white. Sarcoidosis is relatively common in Scandinavia and Northern Ireland, but rare in China, Japan, and Africa. For some reason, those who have moved from a part of the world where the prevalence is low to a part of the world where it is high tend to take on the risk of the higher prevalence area.
What other tests are used to diagnose sarcoidosis?
A variety of tests may be ordered, both to help diagnose sarcoidosis and to determine the degree of organ involvement. Laboratory tests may include a liver panel, complete blood count (CBC), and calcium (both blood and urine levels may be elevated). Other tests may include a physical exam for skin lesions, pulmonary function tests as about 90% of the time there will be some degree of lung involvement, bronchoscopy (a procedure that uses a flexible tube to look at the lining of the airway and to biopsy the lung), chest x-ray, and gallium screening (radioactive gallium is used to evaluate inflammation). Biopsies of the skin, lungs, lymph nodes, and sometimes liver may also be needed, as may a thorough eye exam. A test called a slit-lamp examination may be used.
References- Morris DL, Bhimji SS. Angiotensin II. [Updated 2018 Sep 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499912
- Herman LL, Bhimji SS. Angiotensin Converting Enzyme Inhibitors (ACEI) [Updated 2017 Mar 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431051
- Khanna A, English SW, Wang XS, Ham K, Tumlin J, Szerlip H, Busse LW, Altaweel L, Albertson TE, Mackey C, McCurdy MT, Boldt DW, Chock S, Young PJ, Krell K, Wunderink RG, Ostermann M, Murugan R, Gong MN, Panwar R, Hästbacka J, Favory R, Venkatesh B, Thompson BT, Bellomo R, Jensen J, Kroll S, Chawla LS, Tidmarsh GF, Deane AM., ATHOS-3 Investigators. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017 Aug 03;377(5):419-430 https://www.nejm.org/doi/10.1056/NEJMoa1704154
- Janssens U. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017 Dec 28;377(26):2603-4. https://www.nejm.org/doi/full/10.1056/NEJMc1714511
- John M. Eisenberg Center for Clinical Decisions and Communications Science. ACEIs, ARBs, or DRI for Adults With Hypertension. 2011 Oct 24. In: Comparative Effectiveness Review Summary Guides for Clinicians [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2007-. Figure 1, Different mechanisms of pharmacological blockade of the renin-angiotensin system. Available from: https://www.ncbi.nlm.nih.gov/books/NBK82803/figure/clinacei2.f1
- Pathophysiological regulation of the AT1-receptor and implications for vascular disease. J Hypertens Suppl. 2006 Mar;24(1):S15-21. https://www.ncbi.nlm.nih.gov/pubmed/16601568
- Renal sympathetic nerve activity in the development of hypertension. Curr Hypertens Rep. 2006 Jun;8(3):242-8. https://www.ncbi.nlm.nih.gov/pubmed/17147923
- The renin-angiotensin system in glomerular podocytes: mediator of glomerulosclerosis and link to hypertensive nephropathy. Curr Hypertens Rep. 2006 May;8(2):132-8. https://www.ncbi.nlm.nih.gov/pubmed/16672146
- Renal and vascular hypertension-induced inflammation: role of angiotensin II. Curr Opin Nephrol Hypertens. 2006 Mar;15(2):159-66. https://www.ncbi.nlm.nih.gov/pubmed/16481883
- Brain angiotensin II: new developments, unanswered questions and therapeutic opportunities. Cell Mol Neurobiol. 2005 Jun;25(3-4):485-512. https://www.ncbi.nlm.nih.gov/pubmed/16075377
- Fountain JH, Lappin SL. Physiology, Renin Angiotensin System. [Updated 2017 Dec 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470410/
- Cognitive-enhancing effects of angiotensin IV. BMC Neurosci. 2008;9 Suppl 2(Suppl 2):S15. Published 2008 Dec 3. doi:10.1186/1471-2202-9-S2-S15 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2604899/
- Evidence that the angiotensin IV (AT(4
- The Brain Hepatocyte Growth Factor/c-Met Receptor System: A New Target for the Treatment of Alzheimer’s Disease. J Alzheimers Dis. 2015;45(4):985-1000. doi: 10.3233/JAD-142814. https://www.ncbi.nlm.nih.gov/pubmed/25649658
- The development of small molecule angiotensin IV analogs to treat Alzheimer’s and Parkinson’s diseases. Prog Neurobiol. 2015 Feb;125:26-46. doi: 10.1016/j.pneurobio.2014.11.004. Epub 2014 Nov 29. https://www.ncbi.nlm.nih.gov/pubmed/25455861
- James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC, Svetkey LP, Taler SJ, Townsend RR, Wright JT, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 05;311(5):507-20 https://jamanetwork.com/journals/jama/fullarticle/1791497
- Dagenais GR, Yusuf S, Bourassa MG, Yi Q, Bosch J, Lonn EM, Kouz S, Grover J., HOPE Investigators. Effects of ramipril on coronary events in high-risk persons: results of the Heart Outcomes Prevention Evaluation Study. Circulation. 2001 Jul 31;104(5):522-6
- Heart Outcomes Prevention Evaluation Study Investigators. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N. Engl. J. Med. 2000 Jan 20;342(3):145-53





{kind=link}