What is calcitonin
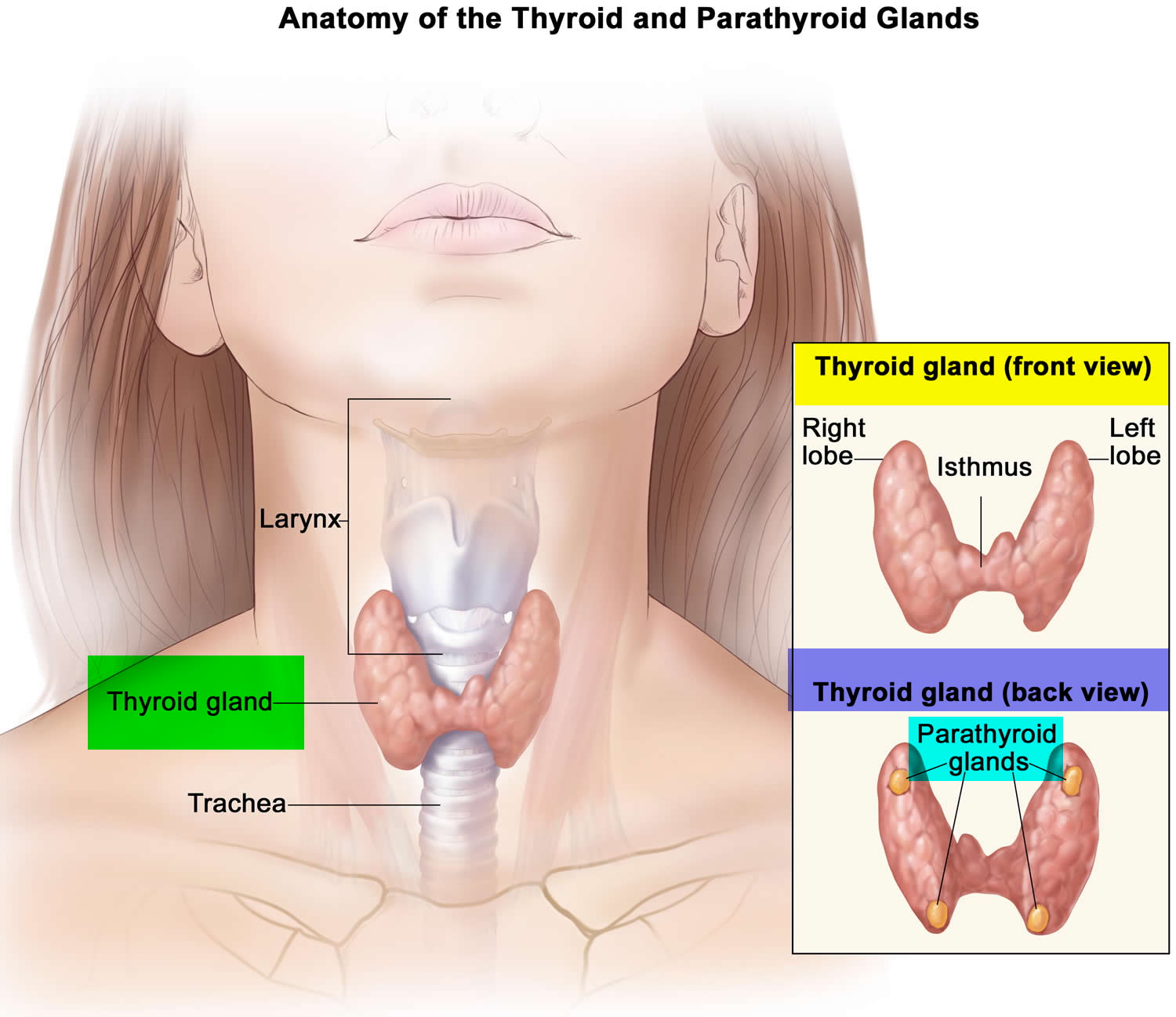
Calcitonin is a hormone produced by special cells in your thyroid gland called C-cells. The thyroid gland is a small butterfly-shaped gland that lies over and flat against the windpipe in the throat. Your thyroid gland produces calcitonin and several hormones that help control the rate of metabolism, primarily thyroxine (T4) and triiodothyronine (T3).
The main action of calcitonin is the regulation of calcium levels in your blood by inhibiting bone breakdown (resorption) by regulating the number and activity of osteoclasts and decreasing kidney reabsorption of calcium. However, calcitonin hormone role in calcium regulation is minor compared with parathyroid hormone (PTH) and 1,25-dihydroxyvitamin D. Thus, the measurement of calcitonin in blood is not useful for diagnosis of disorders of calcium regulation.
In two rare conditions, C-cell hyperplasia and medullary thyroid cancer, excessive amounts of calcitonin are produced. C-cell hyperplasia is a benign condition that may or may not progress to become medullary thyroid cancer. Medullary thyroid cancer is malignant – it can spread beyond the thyroid and can be difficult to treat if it is not discovered early.
Medullary cancer is a rare form of thyroid cancer that accounts for 1-2% of all thyroid cancers in the United States. About 75-80% of medullary thyroid cancer cases are sporadic, occurring in those who do not have a family history of the disease. About 20-25% of cases are related to an inherited mutation in the RET gene that leads to multiple endocrine neoplasia type 2 (MEN 2). MEN 2 is a syndrome associated with several related diseases, including medullary thyroid cancer and pheochromocytomas. The altered RET gene is inherited in an autosomal dominant fashion. Only one copy of the mutated gene – from either a father or mother – is required to have a greatly increased risk of developing medullary thyroid cancer. Most cases of sporadic medullary thyroid cancer develop when people are in their 40s or 50s, and the prevalence is higher in women. The inherited form affects both sexes equally and can occur at an earlier age.
Figure 1. Thyroid gland location
Where is calcitonin produced?
Calcitonin is secreted by by the parafollicular cells (also referred to as calcitonin cells or C cells) of the thyroid and other neuroendocrine cells.
Malignant tumors arising from thyroid C cells (medullary thyroid carcinoma) usually produce elevated levels of calcitonin. Medullary thyroid carcinoma is an uncommon malignant thyroid tumor, comprising less than 5% of all thyroid malignancies. Approximately 25% of these cases are familial, usually appearing as a component of multiple endocrine neoplasia type 2 (MEN 2, Sipple syndrome). Medullary thyroid carcinoma may also occur in families without other associated endocrine dysfunction, with similar autosomal dominant transmission as MEN 2, which is then called familial medullary thyroid carcinoma. Mutations in the RET proto-oncogene are associated with MEN 2 and familial medullary thyroid carcinoma.
Serum calcitonin concentrations are high in infants, decline rapidly, and are relatively stable from childhood through adult life. In general, calcitonin serum concentrations are higher in men than in women due to the larger C-cell mass in men. Serum calcitonin concentrations may be increased in patients with chronic renal failure, and other conditions such as hyperparathyroidism, leukemic and myeloproliferative disorders, Zollinger-Ellison syndrome, autoimmune thyroiditis, small cell and large cell lung cancers, breast and prostate cancer, mastocytosis, and various neuroendocrine tumors, in particular, islet cell tumors.
Figure 2. Thyroid gland anatomy
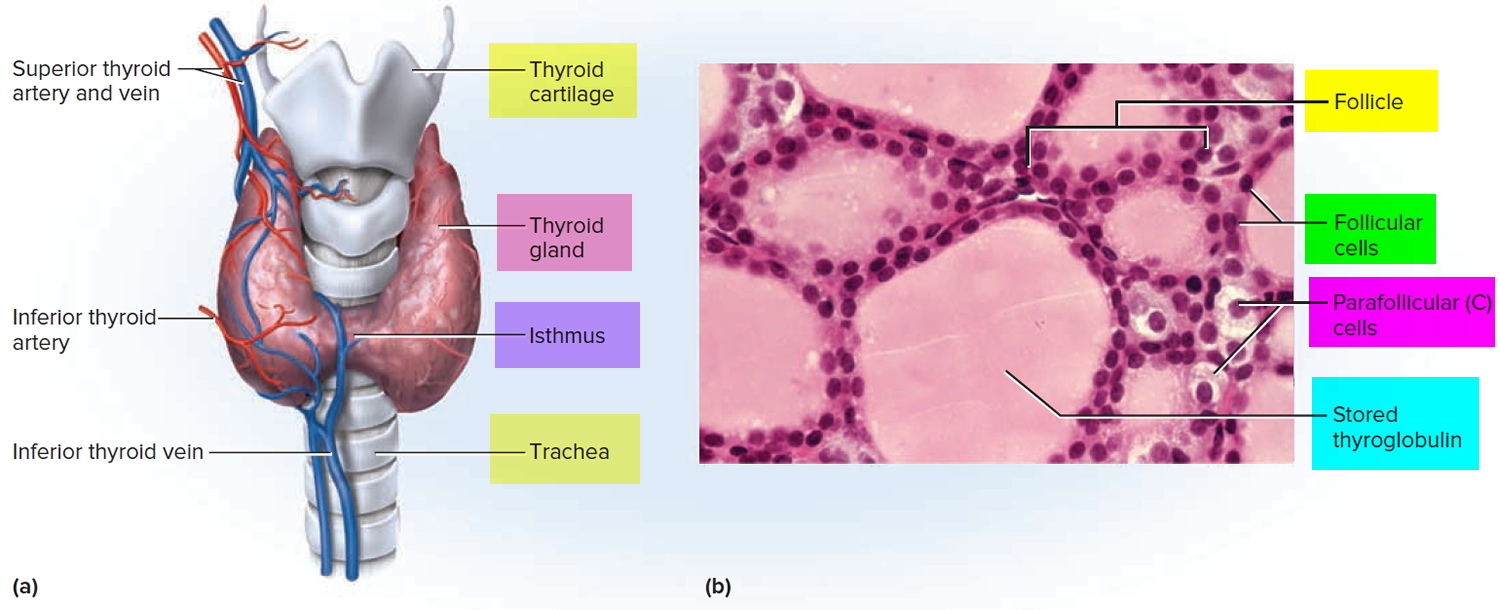
Footnote: (a) Gross anatomy, anterior view. (b) Histology, showing the saccular thyroid follicles (the source of thyroid hormone) and nests of C cells (the source of calcitonin).
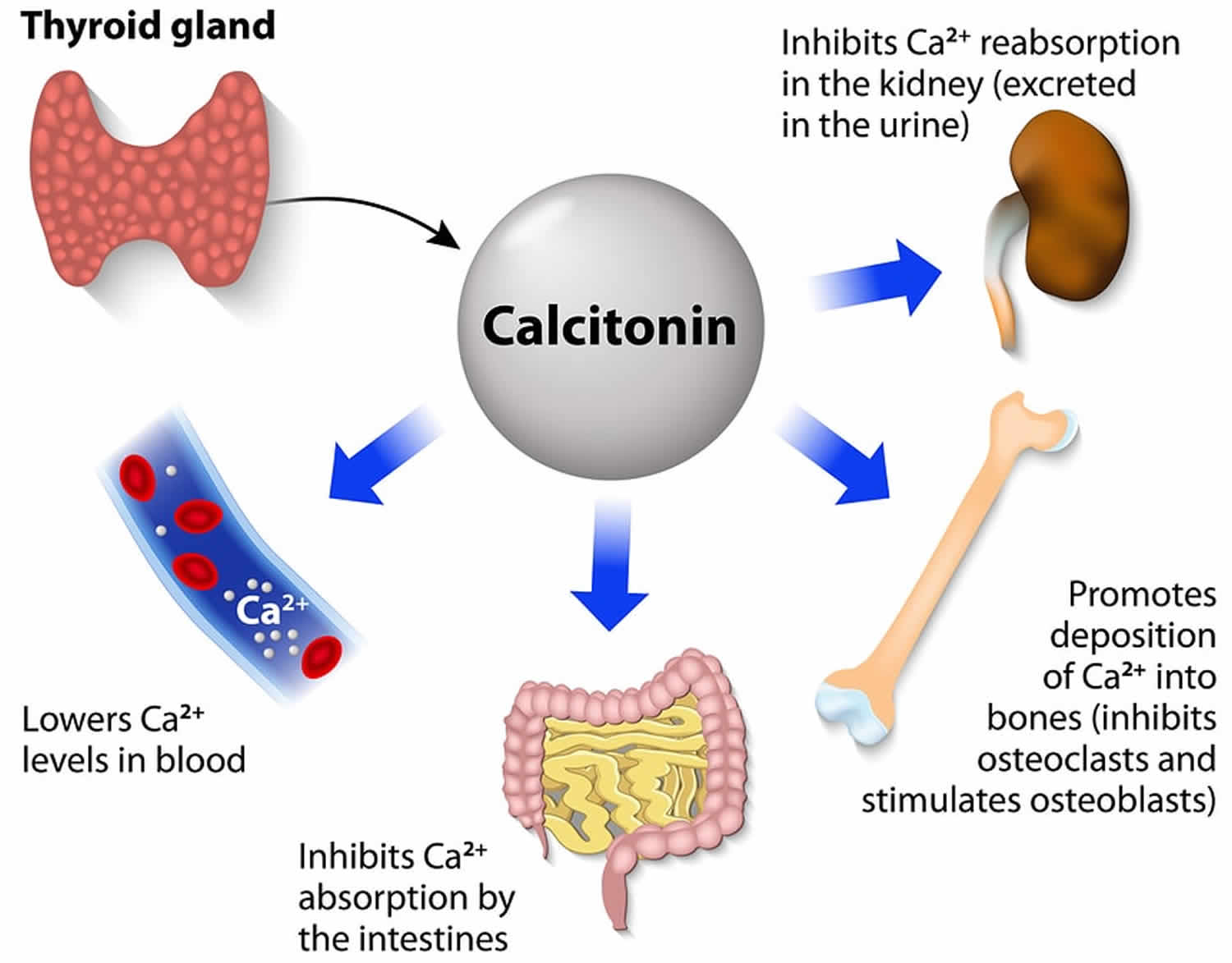
What does calcitonin do?
Calcitonin is a 32-amino acid peptide whose main function is to inhibit osteoclast-mediated bone breakdown (resorption) by regulating the number and activity of osteoclasts 1. Calcitonin is secreted in direct response to serum hypercalcemia and may prevent large oscillations in serum calcium levels and excessive loss of body calcium. However, in comparison to parathyroid hormone and 1,25-dihydroxyvitamin D, the role of calcitonin in the regulation of serum calcium in humans is minor. Measurements of serum calcitonin levels are, therefore, not useful in the diagnosis of disorders of calcium homeostasis.
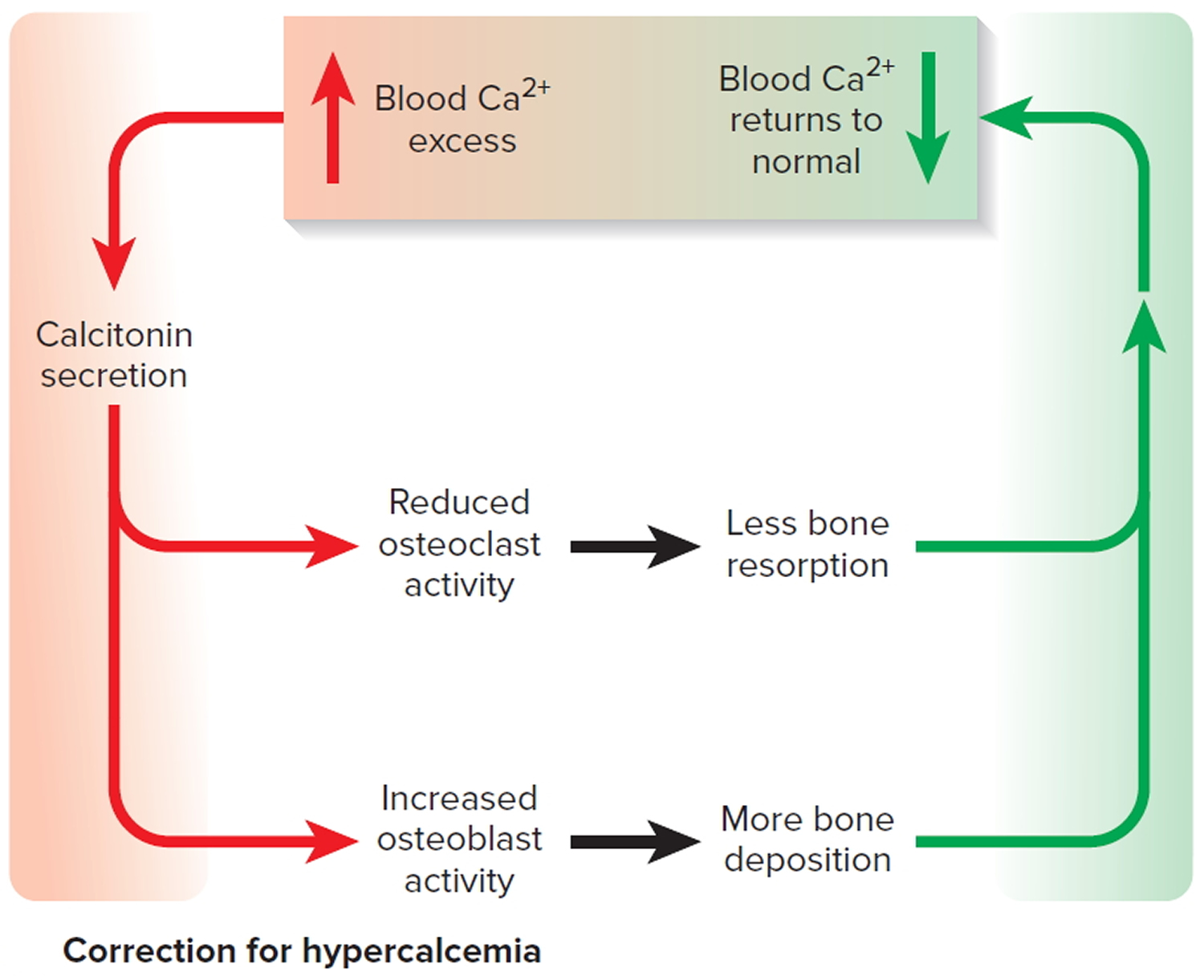
Hypercalcemia (high blood calcium) increases secretion of calcitonin, while hypocalcemia (low blood calcium) inhibits secretion of calcitonin (see Figure 3) 2. Calcitonin secretion is controlled by serum calcium through the same calcium-sensing receptor (CaSR) that regulates parathyroid hormone (PTH) secretion, but in an inverse manner and at higher concentrations of calcium 3. The major effect of calcitonin is to indirectly inhibit bone resorption by inactivating the calcitonin-receptor rich osteoclast. Calcitonin also inhibits the renal reabsorption of phosphate, thus promoting renal phosphate excretion. Calcitonin also induces a mild natriuresis (excretion of sodium in the urine) and calciuresis (excretion of calcium in the urine), the latter contributing to its hypocalcemic effect. However, calcitonin does not appear to have a major effect on human calcium metabolism as evidenced by normocalcemia in thyroidectomized patients as well as patients with medullary thyroid cancer and very high calcitonin levels 4. Calcitonin in pharmacologic doses has been used to decrease bone resorption in osteoporosis, Paget’s bone disease, and hypercalcemia of malignancy, however, there may be an association of long-term use with increased cancer risk 5.
Calcitonin function on mineral metabolism:
- Bone
- Inhibits bone breakdown
- ? Promotes formation
- Kidney
- Increases calcium excretion
- Increases phosphorus excretion
- Gastrointestinal Tract
- ? Inhibitory effect on calcium/phosphorus absorption
- Blood
- Decreases calcium
- Decreases phosphorus
Figure 3. Correction of hypercalcemia (high blood calcium) by calcitonin
Regulation of Calcitonin Secretion
- Calcium and related ions (CaSR)
- Age and gender
- Gastrointestinal factors
The calcitonin receptor, like the PTH and calcium-sensing receptor, is a heptahelical G protein-coupled receptor coupled to the PKA, PKC, and Ca++ signal transduction pathways 4. Several isoforms of the receptor have been identified at different organ sites and may play a tissue-specific effects.
The calcitonin gene through alternative exon splicing and polypeptide processing ultimately encodes two peptide products, calcitonin in thyroid C-cells which is processed from a 141-amino acid precursor, and a 37-amino peptide called calcitonin gene-related peptide (CGRP) in neural tissues which is processed from a 128-amino acid precursor 6. Calcitonin gene-related peptide (CGRP) is weakly recognized by the calcitonin receptor and thereby has a calcitonin-like effect on osteoclasts and osteoblasts. Calcitonin gene-related peptide (CGRP) also acts through its own receptor to produce vasodilation and to act as a neurotransmitter. In addition to its role in calcium and skeletal metabolism, calcitonin is important as a tumor marker in medullary thyroid carcinoma and other neuroendocrine tumors. The receptor that mediates the effects of the peptide products of the calcitonin gene can be modulated by accessory proteins to alter binding characteristics 7.
Calcitonin test
The calcitonin test is primarily used to help diagnose C-cell hyperplasia and medullary thyroid cancer, to evaluate the effectiveness of treatment, and to monitor those affected for recurrence. It is also ordered to screen for medullary thyroid cancer in family members of people with multiple endocrine neoplasia type 2 (MEN 2).
C-cell hyperplasia and medullary thyroid cancer are two rare conditions in which excessive amounts of calcitonin are produced. C-cell hyperplasia is a benign condition that may or may not progress to become medullary thyroid cancer. Medullary thyroid cancer is malignant – it can spread beyond the thyroid and can be difficult to treat if it is not discovered early.
Stimulation tests are more sensitive than calcitonin measurements alone. This involves collecting a baseline sample, then giving a person an injection of intravenous calcium or pentagastrin to stimulate calcitonin production. Several more blood samples are then collected over the next few minutes to measure the effect of the stimulation. People with early C-cell hyperplasia and/or medullary thyroid cancer will usually have very significant increases in their levels of calcitonin during this test.
When is calcitonin test ordered?
A common reason to have the test is if you have had surgery to remove a thyroid tumor called medullary cancer. The test allows your health care provider to evaluate if the tumor has spread (metastasized) or has come back (tumor recurrence).
Calcitonin levels may also be ordered when someone is suspected of having C-cell hyperplasia, medullary thyroid cancer or multiple endocrine neoplasia (MEN) syndrome, or a family history of these conditions. A person may experience signs and symptoms, such as:
- A lump or swelling at the front of the neck
- Pain at the throat or front of the neck
- A change in the voice, hoarseness
- Difficulty swallowing or breathing
- Persistent cough not associated with a cold
A recent study also recommended measuring calcitonin before surgery in all people with thyroid nodules, but not all clinicians agree. Stimulation tests may be ordered when someone has indeterminate or normal calcitonin results but clinical suspicions remain.
Calcitonin tests may be periodically performed on family members of those who have multiple endocrine neoplasia type 2 (MEN 2), starting at an early age, in order to detect medullary thyroid cancer or C-cell hyperplasia as early as possible. When someone has been treated for medullary thyroid cancer, calcitonin testing will usually be ordered at regular intervals to monitor treatment effectiveness and recurrence.
Calcitonin may also be higher in other tumors, such as:
- Insulinoma (tumor in the pancreas that produces too much insulin)
- Lung cancer
- VIPoma (cancer that usually grows from islet cells in the pancreas)
Normal calcitonin levels
Adults
- 17 years and older:
- Males: < or =14.3 pg/mL
- Females: < or =7.6 pg/mL
Pediatric
- 1 month: < or =34 pg/mL
- 2 months: < or =31 pg/mL
- 3 months: < or =28 pg/mL
- 4 months: < or =26 pg/mL
- 5 months: < or =24 pg/mL
- 6 months: < or =22 pg/mL
- 7 months: < or =20 pg/mL
- 8 months: < or =19.0 pg/mL
- 9 months: < or =17.0 pg/mL
- 10 months: < or =16.0 pg/mL
- 11 months: < or =15.0 pg/mL
- 12-14 months: < or =14.0 pg/mL
- 15-17 months: < or =12.0 pg/mL
- 18-20 months: < or =10.0 pg/mL
- 21-23 months: < or =9.0 pg/mL
- 2 years: < or =8.0 pg/mL
- 3-9 years: < or =7.0 pg/mL
- 10-15 years: < or =6.0 pg/mL
- 16 years: < or =5.0 pg/mL
Women and men can have different normal values, with men having higher values.
Sometimes, calcitonin in the blood is checked several times after you are given a shot (injection) of a special medicine that stimulates calcitonin production.
You will need this extra test if your baseline calcitonin is normal, but your provider suspects you have medullary cancer of the thyroid.
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or may test different specimens. Talk to your provider about the meaning of your specific test results.
What abnormal calcitonin results mean
Higher-than-normal levels of calcitonin can also occur in people with kidney disease, smokers, and higher body weight. Also, it increases when taking certain medicines to stop stomach acid production.
A higher-than-normal level may indicate:
- Insulinoma
- Lung cancer
- Medullary cancer of thyroid (most common)
- Breast cancer
- Pancreatic cancer
- VIPoma rare pancreatic tumor associated with vasoactive intestinal peptide (VIP) hormone production
Other conditions with elevated calcitonin include:
- Intestinal, gastric, or bronchial carcinoid tumors
- Chronic renal failure
- Zollinger-Ellison syndrome
- Pernicious anemia
Although most patients with sporadic medullary thyroid carcinoma have high basal serum calcitonin concentrations, 30% of those with familial medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (MEN 2) have normal basal levels.
In completely cured cases following surgical therapy for medullary thyroid carcinoma, serum calcitonin levels fall into the undetectable range over a variable period of several weeks. Persistently elevated postoperative serum calcitonin levels usually indicate incomplete cure. The reasons for this can be locoregional lymph node spread or distant metastases. In most of these cases, imaging procedures are required for further workup. Those individuals who are then found to suffer only locoregional spread may benefit from additional surgical procedures. However, the survival benefits derived from such approaches are still debated.
A rise in previously undetectable or very low postoperative serum calcitonin levels is highly suggestive of disease recurrence or spread, and should trigger further diagnostic evaluations.
Cautions
Calcitonin test is not useful for evaluating calcium metabolic diseases.
Samples should not be taken from patients receiving therapy with high biotin or vitamin B7 doses (i.e., >5 mg/day) until at least 12 hours following the last biotin administration.
Falsely elevated values may occur in serum from patients who have developed human antimouse antibodies or heterophilic antibodies.
In rare cases, interference due to extremely high titers of antibodies to analyte-specific antibodies, streptavidin, or ruthenium can occur.
Values obtained with different assay methods or kits may be different and cannot be used interchangeably. Test results cannot be interpreted as absolute evidence for the presence or absence of malignant disease.
Is there anything else I should know?
With medullary thyroid cancer and C-cell hyperplasia, other thyroid tests, such as T4, T3, and TSH, are usually normal while calcitonin levels are elevated.
Concentrations of calcitonin may be increased with use of drugs such as epinephrine, glucagon, and oral contraceptives, and are normally higher in newborns as well as in women during pregnancy.
Calcitonin medication
Calcitonin Salmon Nasal Spray
Calcitonin salmon nasal spray is a man-made form (from salmon) of calcitonin hormone that occurs naturally in the thyroid gland. Calcitonin salmon works by preventing bone breakdown and increasing bone density (thickness). Calcitonin nasal spray is used to treat osteoporosis in women who are at least 5 years past menopause and cannot or do not want to take estrogen products. Osteoporosis is a disease that causes bones to weaken and break more easily. Calcitonin is a human hormone that is also found in salmon. Calcitonin nasal spray is used together with calcium and vitamin D.
How should calcitonin nasal be used?
Calcitonin salmon comes as a spray to be used in the nose. It is usually used once a day, alternating nostrils every day. To help you remember to use calcitonin salmon, use it around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Use calcitonin salmon exactly as directed. Do not use more or less of it or use it more often than prescribed by your doctor.
Calcitonin salmon helps treat osteoporosis but does not cure it. Continue to use calcitonin salmon even if you feel well. Do not stop using calcitonin salmon without talking to your doctor.
Before using calcitonin salmon nasal spray the first time, read the written instructions that come with it. Ask your doctor or pharmacist to show you how to use it. Practice using the nasal spray while he or she watches.
To put the pump and bottle together, remove the rubber stopper from the bottle, and then remove the plastic protective cap from the bottom of the spray unit. Put the spray pump into the bottle and turn to tighten. Then take the plastic cover off of the top of the spray unit.
Before the first time you use a new bottle, you need to prime (activate) the pump. To prime the pump, follow these steps:
- Allow the bottle to reach room temperature.
- Hold the bottle upright, and press down on the two white side arms of the pump at least 5 times, until a full spray is produced. The pump is now primed.
To use the calcitonin salmon nasal spray, follow these steps:
- Keep your head up and place the nozzle in one nostril.
- Press down on the pump to release the calcitonin salmon.
- Use the opposite nostril each day.
- Each bottle has enough medication for 30 doses.
What special precautions should I follow?
Before using calcitonin salmon nasal spray:
- tell your doctor and pharmacist if you are allergic to calcitonin salmon or any other medications. Your doctor may do a skin test before you start calcitonin salmon to make sure you do not have an allergic reaction to it.
- tell your doctor and pharmacist what prescription and nonprescription medications, vitamins, nutritional supplements, and herbal products you are taking.
- tell your doctor if you are pregnant, plan to become pregnant, or are breast-feeding. If you become pregnant while using calcitonin salmon, call your doctor.
The presence of other medical problems may affect the use of this medicine. Make sure you tell your doctor if you have any other medical problems, especially:
- Paget’s disease—Use with caution. Some medicines used for this condition (eg, alendronate, etidronate, or risedronate) may keep calcitonin nasal spray from working properly.
- Hypocalcemia (low calcium levels) or
- Vitamin D deficiency—Must be treated first before using this medicine.
Other precautions
It is very important that your doctor check your progress at regular visits to make sure that this medicine is working properly. Blood and urine tests may be needed to check for unwanted effects. Your doctor may also want to check your nose before and during treatment with this medicine.
Your doctor might give you an allergy skin test to see if you are allergic to calcitonin before using this medicine.
This medicine may cause serious allergic reactions, including anaphylaxis. Anaphylaxis can be life-threatening and requires immediate medical attention. The most serious signs of this reaction are rash, itching, hoarseness, trouble breathing, trouble swallowing, or any swelling of your hands, face, or mouth while you are using this medicine. If these side effects occur, get emergency help at once.
This medicine can lower your calcium levels in the blood (hypocalcemia). Check with your doctor right away if you have abdominal or stomach cramps, confusion, convulsions, difficulty breathing, mood or mental changes, muscle cramps in hands, arms, feet, legs, or face, or numbness and tingling around the mouth, fingertips, or feet.
This medicine may cause irritation in the nose that can be painful and serious. Check with your doctor right away if you have more than one of the following symptoms: sneezing, runny or stuffy nose, shortness of breath, troubled breathing, or heavy nosebleeds.
This medicine may increase your risk of having cancer. Talk to your doctor if you have concerns about this risk.
Do not take other medicines unless they have been discussed with your doctor. This includes prescription or nonprescription (over-the-counter [OTC]) medicines and herbal or vitamin supplements.
What special dietary instructions should I follow?
It is important that you get enough calcium and vitamin D while you are using calcitonin salmon. Your doctor may prescribe supplements if your dietary intake is not enough.
Calcitonin salmon nasal spray dosage
The dose of this medicine will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of this medicine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
- For nasal dosage form (spray):
- Postmenopausal osteoporosis:
- Adults—200 International Units (IU) or 1 spray into one nostril per day. It is best to change which nostril you use each day. As an example, you should spray into the left side on the first day, then into the right side on the second day, and back to the left side on the third day.
- Children—Use and dose must be determined by your doctor.
- Postmenopausal osteoporosis:
What should I do if I forget a dose?
Apply the missed dose as soon as you remember it. However, if it is almost time for the next dose, skip the missed dose and continue your regular dosing schedule. Do not use a double dose to make up for a missed one.
What side effects can calcitonin salmon nasal spray cause?
More common
- back pain
- joint pain
Calcitonin salmon nasal spray may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- runny nose
- nosebleed
- sinus pain
- nose symptoms such as crusts, dryness, redness, or swelling
- back pain
- joint pain
- upset stomach
- flushing (feeling of warmth)
Less common or rare
- abdominal or stomach pain
- body aches
- burning, dry, or itching eyes
- constipation
- flushing
- mental depression
- muscle pain
- nausea
- unusual tearing of the eyes
- upset stomach
Incidence not known
- continuing ringing or buzzing or other unexplained noise in the ears
- hearing loss
- trouble hearing
- trouble seeing
Some side effects can be serious. The following symptoms are uncommon, but if you experience any of them, see your doctor immediately:
- hives
- skin rash
- itching
- difficulty breathing or swallowing
- swelling of the tongue or throat
Call your doctor at once if you have:
- a light-headed feeling, like you might pass out;
- severe nasal irritation; or
- low levels of calcium in your blood–numbness or tingly feeling around your mouth, fast or slow heart rate, muscle tightness or contraction, overactive reflexes.
Calcitonin salmon nasal spray may cause other side effects. Call your doctor if you have any unusual problems while using this medication.
Calcitonin Salmon Injection
Calcitonin salmon injection is used to treat osteoporosis in postmenopausal women. Osteoporosis is a disease that causes bones to weaken and break more easily. Calcitonin salmon injection is also used to treat Paget’s disease of bone and to quickly reduce calcium levels in the blood when needed.
Calcitonin salmon injection may increase your risk of having a cancer. Talk with your doctor about this risk.
How should calcitonin salmon injection be used?
Calcitonin salmon comes as a solution to be injected under the skin (subcutaneously) or into the muscle (intramuscularly). Calcitonin salmon injection is usually used once a day or once every other day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Use calcitonin salmon injection exactly as directed. Do not use more or less of it or use it more often than prescribed by your doctor.
Your doctor, nurse, or pharmacist will show you how to administer the medication. Follow all directions carefully. Dispose of all empty syringes and vials as directed by your healthcare provider.
Before preparing a dose, look at the vial. If the solution is discolored or contains particles, do not use it, and call your pharmacist.
Calcitonin salmon helps treat osteoporosis and Paget’s disease of bone but does not cure them. Continue to use calcitonin salmon even if you feel well. Do not stop using calcitonin salmon without talking to your doctor.
Other uses for calcitonin salmon injection
Calcitonin salmon injection is also used sometimes to treat osteogenesis imperfecta. Talk to your doctor about the possible risks of using this medication for your condition. Calcitonin salmon injection may be prescribed for other uses; ask your doctor or pharmacist for more information.
What special precautions should I follow?
Before using calcitonin salmon injection:
- tell your doctor and pharmacist if you are allergic to calcitonin salmon or any other medications. Your doctor may do a skin test before you start calcitonin salmon to make sure you do not have an allergic reaction to it.
- tell your doctor and pharmacist what prescription and nonprescription medications, vitamins, nutritional supplements, and herbal products you are taking.
- tell your doctor if you are pregnant, plan to become pregnant, or are breast-feeding. If you become pregnant while using calcitonin salmon, call your doctor.
The presence of other medical problems may affect the use of this medicine. Make sure you tell your doctor if you have any other medical problems, especially:
- Hypocalcemia (low calcium in the blood)—Use with caution. May make this condition worse.
- Vitamin D deficiency—Must be treated first before using this medicine.
What special dietary instructions should I follow?
If you are using this medicine for hypercalcemia (too much calcium in the blood), your doctor may want you to follow a low-calcium diet. If you have any questions about this, check with your doctor.
If you are using this medicine for postmenopausal osteoporosis, your doctor may also want you to take calcium and vitamin D every day. If you have any questions about this, check with your doctor.
Calcitonin salmon injection dosage
The dose of this medicine will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of this medicine. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
- For injection dosage form:
- Paget’s disease of the bone:
- Adults—100 International Units (IU) or 0.5 milliliter (mL) injected into a muscle or under the skin once a day. Your doctor may adjust your dose as needed.
- Children—Use and dose must be determined by your doctor.
- Hypercalcemia:
- Adults—Dose is based on body weight and must be determined by your doctor. The starting dose is 4 International Units (IU) per kilogram (kg) of body weight injected into a muscle or under the skin every 12 hours. Your doctor may adjust your dose as needed. However, the dose is usually not more than 8 IU per kg of body weight every 6 hours.
- Children—Use and dose must be determined by your doctor.
- Postmenopausal osteoporosis:
- Adults—100 International Units (IU) or 0.5 milliliter (mL) injected into a muscle or under the skin every other day.
- Children—Use and dose must be determined by your doctor.
- Paget’s disease of the bone:
What should I do if I forget a dose?
Do not administer a double dose to make up for a missed one. Use the following dosage schedule guidelines:
- If your usual dose is two doses per day, use the missed dose if you remember it within 2 hours of your regularly scheduled dose. Otherwise, skip the missed dose and then continue on the regular dosing schedule.
- If your usual dose is one dose per day, use the missed dose if you remember it during the same day. Otherwise, skip the missed dose and continue the regular dosing schedule the next day.
- If your usual dose is every other day, use the missed dose as soon as you remember it, either on the regularly scheduled day or the next day. Then, continue a regular dosing schedule of every other day from that point.
- If your usual dose is three times a week, give the missed dose on the next day and continue every other day thereafter. Resume the regular dosing schedule at the beginning of the next week.
What side effects can calcitonin salmon injection cause?
More common
- red streaks on the skin
- swelling, tenderness, or pain at the injection site
Less common
- feeling of warmth
- redness of the face, neck, arms, and occasionally, upper chest
Calcitonin salmon injection may cause side effects. Tell your doctor if any of these symptoms are severe or do not go away:
- upset stomach
- vomiting
- redness, swelling, or irritation at the site of injection
- flushing (feeling of warmth) of the face or hands
- increased urination at night
- itching of the ear lobes
- feverish feeling
- eye pain
- decreased appetite
- stomach pain
- swelling of the feet
- salty taste
Some side effects can be serious. The following symptoms are uncommon, but if you experience any of them, call your doctor immediately:
- hives
- skin rash
- itching
- difficulty breathing or swallowing
- swelling of the tongue or throat
Check with your doctor immediately if any of the following side effects occur:
Incidence not known
- Blurred vision
- chills or fever
- cough
- difficulty with breathing
- difficulty with swallowing
- dizziness
- frequent urination
- headache
- joint pain
- muscle aches and pains
- muscle cramps in the hands, arms, feet, legs, or face
- nausea or vomiting
- puffiness or swelling of the eyelids or around the eyes, face, lips, or tongue
- seizures
- skin rash or itching
- slow or fast heartbeat
- sweating
- swelling of the hands, ankles, feet, or lower legs
- tightness in the chest
- tingling of the hands or feet
- trembling or shaking of the legs, arms, hands or feet
- trouble sleeping
- unusual tiredness or weakness
- unusual weight gain or loss
Some side effects may occur that usually do not need medical attention. These side effects may go away during treatment as your body adjusts to the medicine. Also, your health care professional may be able to tell you about ways to prevent or reduce some of these side effects. Check with your health care professional if any of the following side effects continue or are bothersome or if you have any questions about them:
Incidence not known
- abdominal or stomach pain
- changes in vision
- diarrhea
- pain in the eyes
- poor appetite
- waking to urinate at night
Other side effects not listed may also occur in some patients. If you notice any other effects, check with your healthcare professional.
Calcitonin salmon may cause other side effects. Call your doctor if you have any unusual problems while taking this medication.
References- Deftos LJ and Gagel R: Calcitonin and Medullary Thyroid Carcinoma In: Cecil Textbook of Medicine, Twentieth First Edition, JB Wyngarden and JC Bennett, Chapter 265, pp.1406-1409, 2000.
- Deftos LJ, Weisman MH, Williams GW, et al. Influence of age and sex on plasma calcitonin in human beings. N Engl J Med 302:1351-1353, 1980.
- Shaker JL, Deftos L. Calcium and Phosphate Homeostasis. [Updated 2018 Jan 19]. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279023
- Watts NB. Estrogens, Estrogen agonists/antagonists, and calcitonin. In Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 8th Edition, Rosen CJ (ed); Chapter 48, pp. 408-411, 2013
- Medicines and Healthcare products Regulatory Agency. Calcitonin (Miacalcic): increased risk of cancer with long-term use. Published: 20 August 2012
- McLatchie LM, Fraser NJ, Main MJ, et al. RAMPs regulate the transport and ligand specificity of the calcitonin-receptor-like receptor. Nature 393:333-339, 1998.
- Muff R, Born W, Fischer JA. Calcitonin, calcitonin gene-related peptide, adrenomedullin and amylin: homologous peptides, separate receptors and overlapping biological actions. Eur J Endocrinol 133:17-20, 1995.





{kind=link}