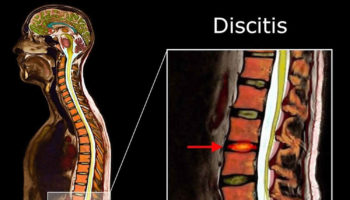
What is discitis Discitis is an inflammation or infection of the intervertebral disc or intervertebral disc space. Discitis can be caused by bacteria, virus, or fungus. Discitis
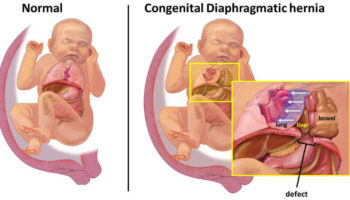
What is a diaphragmatic hernia A diaphragmatic hernia is also called congenital diaphragmatic hernia, is a birth defect in which there is an abnormal opening
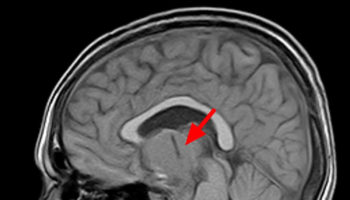
What is craniopharyngioma Craniopharyngiomas are rare benign (noncancerous) tumors that are typically found near the pituitary gland and hypothalamus, which are positioned beneath the center
Corneal transplant surgery A corneal transplant also known as keratoplasty, is a surgical procedure that replaces a disc-shaped segment of an unhealthy cornea with a similarly
What is cryosurgery Cryosurgery is also called cryotherapy, is a medical procedure that uses intense cold produced by liquid nitrogen (or argon gas) to destroy
What is calcification Calcification is a process in which calcium builds up in body tissue, causing the tissue to harden. Calcification can be a normal
{kind=link}



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}