Double aortic arch
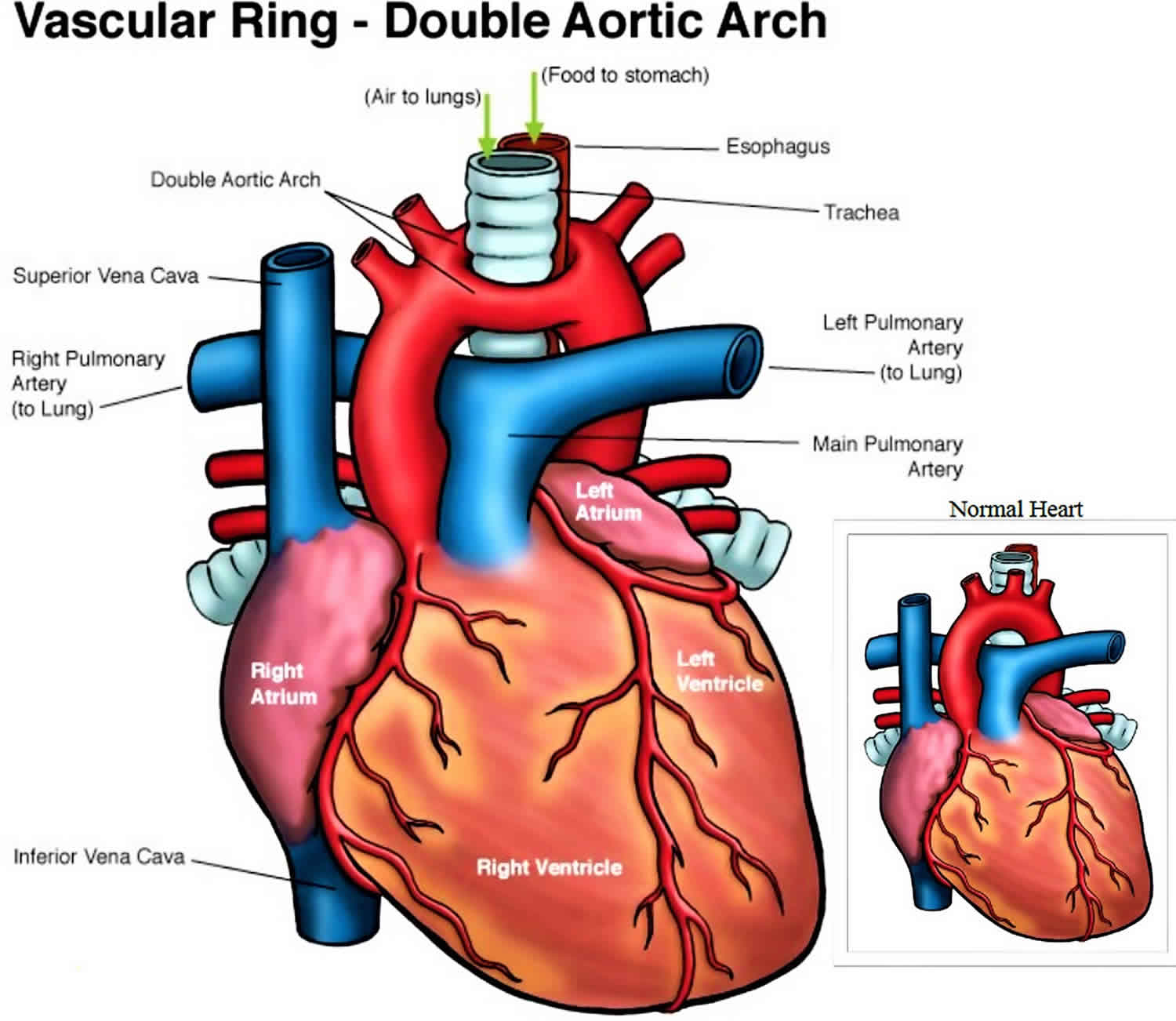
Double aortic arch is a congenital (present at birth) abnormal formation of the aorta, where both the left and right aortic arches are present, resulting in a complete circle around the trachea and esophagus 1. Double aortic arch is the most common cause of tracheoesophageal compression, with an incidence of 46% to 76% in reports of vascular rings 2.
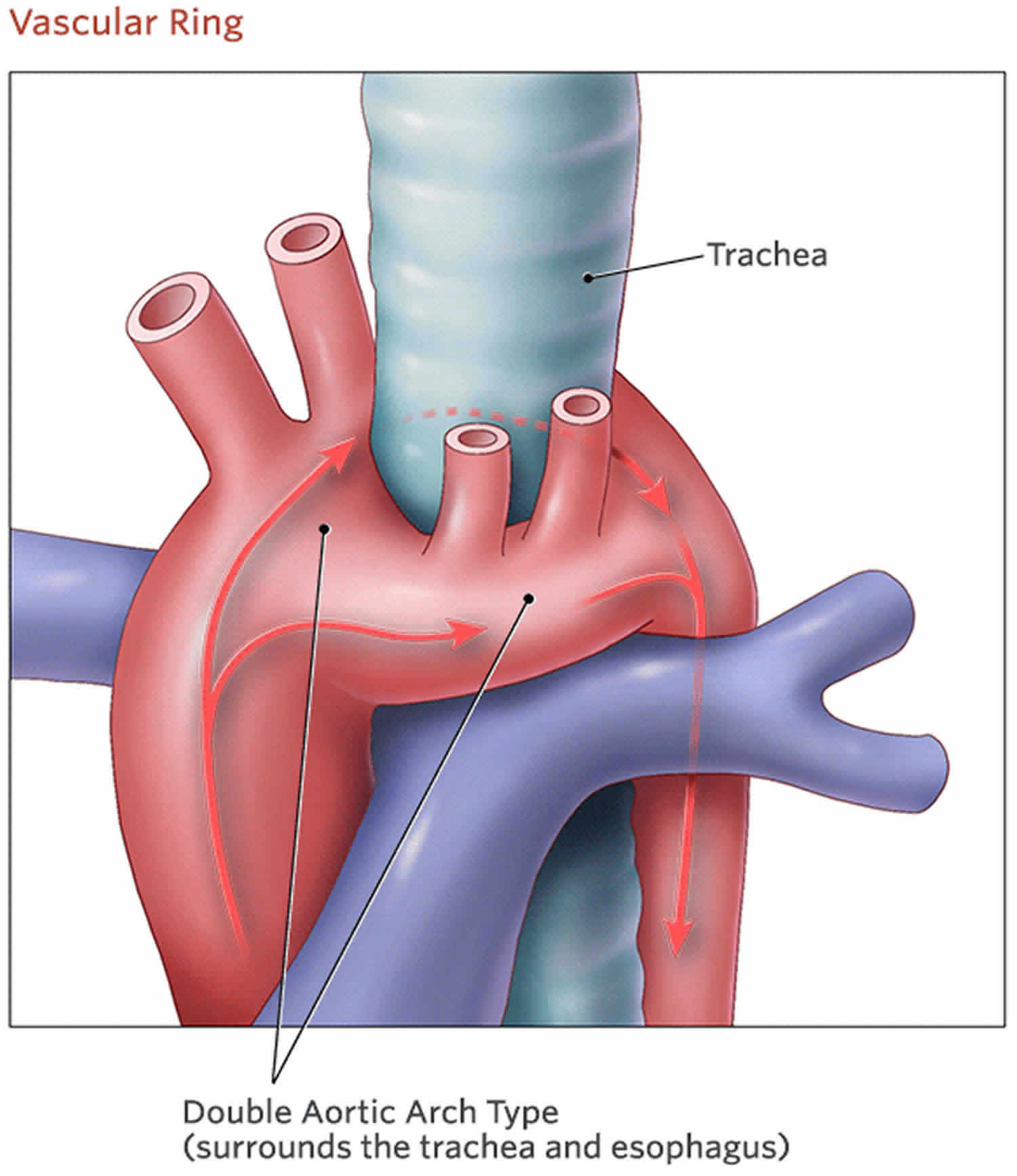
The fetal heart starts with two symmetrical branches of the aorta. Parts of the aortic arch regress in the second month of fetal life, usually resulting in a left aortic arch with three artery branches: the innominate artery, the left common carotid artery, and the left subclavian artery. The ductus arteriosus is present from the left pulmonary artery to the aorta, near the left subclavian origin. Double aortic arch occurs when there is abnormal regression of parts of the original two aortic arch branches. A left and a right aortic arch are present, resulting in a complete circle around the trachea and esophagus. The right aortic arch is usually larger than the left aortic arch. The right arch gives rise to the right common carotid artery and right subclavian artery and the left arch gives rise to the left common carotid artery and left subclavian artery.
Generally, incidence of double aortic arch and vascular rings is unknown, although vascular rings comprise an estimated 1% of cardiovascular malformations that are managed surgically. In most surgical series, 45-65% of patients undergoing repair of a vascular ring have a double aortic arch 1.
Figure 1. Double aortic arch
Double aortic arch causes
A persistent double aortic arch occurs when abnormal regression of the embryonic aortic arch segments is present, in which both the left and right aortic arches remain intact. With the different forms of double aortic arch, different segments of the embryonic aortic arch system, which normally regress, remain patent.
Factors responsible for the aberrant persistence of certain aortic arch segments have not been clearly identified, and the pathogenesis of this anomaly remains a mystery. Double aortic arch typically occurs without associated cardiovascular defects, although other lesions may be present, and accordingly, it is not usually found as part of a syndromic complex.
In a study at the author’s institution, band 22q11 deletions were found in 3 of 22 patients (14%) with double aortic arch 3. This chromosomal anomaly is associated with aortic arch anomalies in patients with other forms of conotruncal heart disease and other isolated vascular abnormalities, and band 22q11 deletion is likely to be an important etiologic factor in double aortic arch. Most such mutations arise de novo, and no recognizable inheritance pattern is present.
Familial recurrence of double aortic arch has been reported, supporting a genetic etiology for this anomaly. Teratogen-induced double aortic arch in animal models also has been reported. The mechanisms and significance of these models have not been elucidated.
Double aortic arch symptoms
Many infants and children with double aortic arch are asymptomatic. Symptoms in patients with double aortic arch depends on several factors, including the severity of tracheal compression, esophageal compression, or both and whether associated anomalies are present. Children with double aortic arch tend to have symptoms sooner and in greater severity than children with right aortic arch with left ligamentum arteriosum. Inspiratory stridor and feeding problems occur in infancy. History of pneumonia is common. Cardiac exam is normal, unless other congenital heart disease is present. Respiratory symptoms may worsen while feeding or in the setting of respiratory infections. Older children my describe food getting “stuck” as they swallow or have frequent coughing/choking while eating.
The following symptoms may be present in children with double aortic arch:
- Noisy or labored breathing, especially with eating
- Difficulty eating and swallowing: the child regurgitates milk or other food
- Dysphagia: the child feels like something is “stuck in the throat”; the child keeps choking or feels like he or she is choking on food
- Persistent cough
- Acid reflux
Double aortic arch diagnosis
In most cases, the symptoms of double aortic arch are mild. That means double aortic arch may go undiagnosed until your child is older, or even an adult. If the condition is severe and your child has trouble breathing, a double aortic arch may be diagnosed at several weeks or months of age.
Diagnosis of a double aortic arch may require some or all of these tests:
- Chest X-ray
- Cardiac Magnetic Resonance Imaging (MRI): a three-dimensional image that shows heart and vessel abnormalities
- Chest CT (CAT scan)
- Echocardiogram : sound waves create an image of the heart, helpful in confirming diagnosis of vascular ring and diagnosis of other congenital heart disease, if present.
- Bronchoscopy: a doctor looks at the trachea using an instrument called a bronchoscope (while patient is under anesthesia)
- Gastrointestinal tests such as barium swallow or barium esophagram. Barium (contrast) fluid is consumed by mouth and coats the esophagus. Fluoroscopy (x-ray) is done at the same time the barium is consumed, which reveals compression or obstruction of the esophagus
Double aortic arch treatment
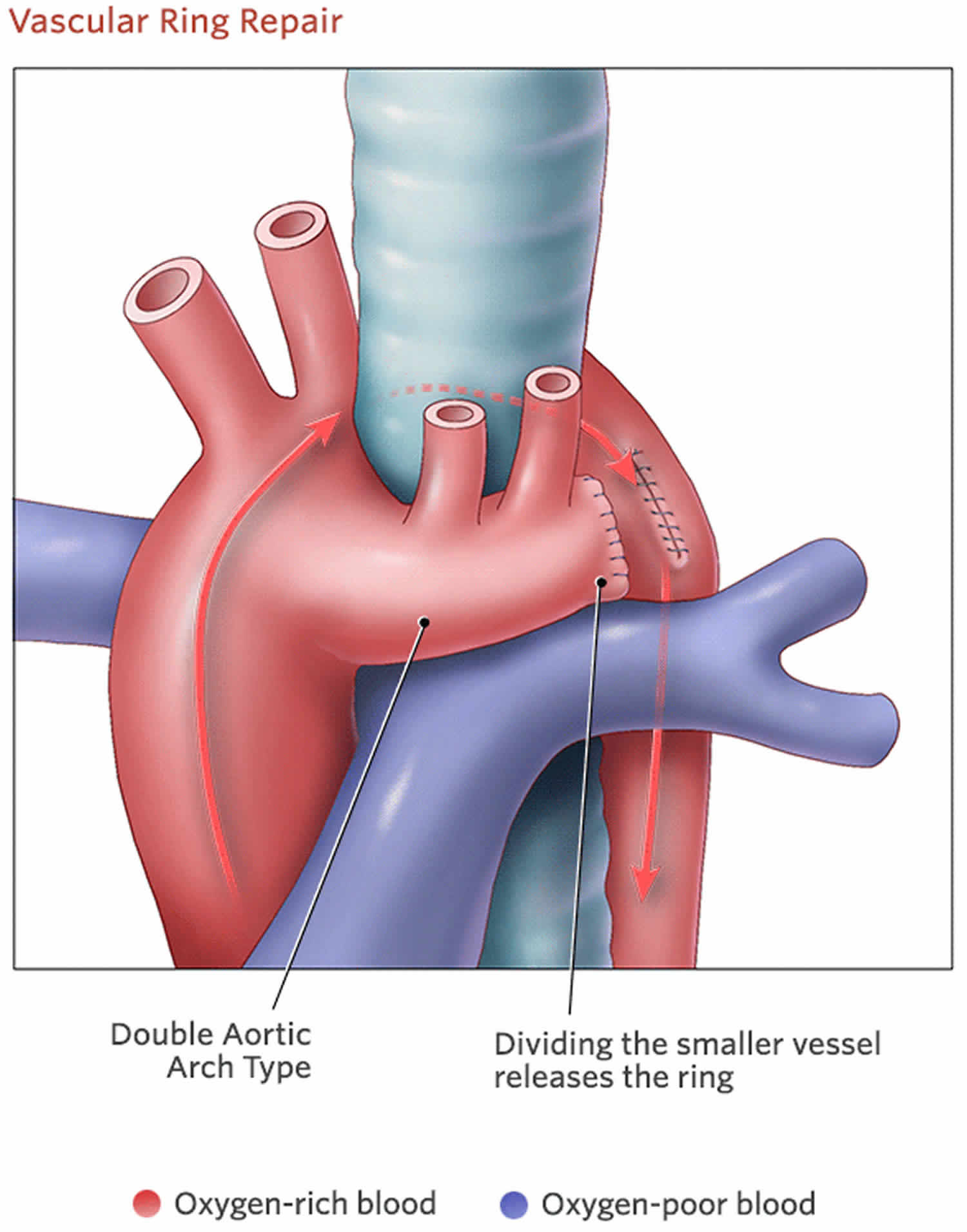
Children with double aortic arch that are asymptomatic do not require surgical intervention. Timing of surgical intervention is determined by the severity of associated symptoms. Double aortic arch requires surgery (not open heart) if there are symptoms. In most cases, the surgeon makes an incision on the left side of the chest and goes between the ribs to access the area. The surgeon will cut and stitch closed one of the arches (usually the left) so the aorta no longer encircles or puts pressure on the trachea or esophagus. Children need careful respiratory management in the postoperative period. Normal life expectancy and development for children without other congenital anomalies.
Figure 2. Double aortic arch repair
Follow-up care
Through age 18
In most cases, children with double aortic arch recover completely after surgery and won’t need additional procedures. It is not uncommon for noisy breathing to continue for several weeks or months after surgery as the trachea slowly takes on a more normal shape. Rarely, symptoms such as coughing or labored breathing continue after surgery. Your child’s surgeon will monitor your child to make sure recovery is as complete and rapid as possible.
Pediatric cardiologists will follow your child until she is a young adult, coordinating care with her primary care physician. She will need to carefully follow doctors’ advice. In rare cases, pediatric cardiologists will suggest that your child limit certain types of exercise.
Into adulthood
Children born with double aortic arch who do not require surgery should follow up with a cardiologist.
Double aortic arch prognosis
Long-term prognosis for patients with repaired double aortic arch is excellent; persistent respiratory symptoms are the most common adverse outcomes.
In patients with a repaired double aortic arch, lifestyle implications are minimal and most likely are related to residual symptoms or associated anomalies.
Morbidity and mortality
The natural history of double aortic arch is not well defined. Vascular rings were among the first congenital cardiovascular anomalies repaired surgically, and surgical management has been the standard of care for more than 50 years. Patients with significant airway compression may die as a result of respiratory compromise, but such events are rare.
Preoperative morbidity generally is limited to respiratory symptoms, feeding problems, or both. Some patients may develop recurrent respiratory infections, and some may exhibit failure to thrive as the result of a combination of increased metabolic requirements from respiratory and feeding work and relatively poor oral intake.
Double aortic arch complications
Complications are uncommon after repair of vascular rings.
The major postoperative symptom is persistent respiratory symptoms, including cough, dyspnea, and wheezing. Pulmonary function testing reveals persistent upper airway obstruction in some patients. Others have evidence of lower airway obstruction that usually is responsive to bronchodilator therapy. Whether the incidence of lower airway obstruction is higher in patients who have undergone repair of vascular rings than in the population at large or whether such a pathologic condition in patients with rings has any relationship to prior anatomic and functional abnormalities is not known.
Rarely, patients with unrepaired double aortic arch may develop an aortoesophageal fistula, which causes fatal hemorrhage. Another rare complication is esophageal erosion.
References- Double aortic arch. https://emedicine.medscape.com/article/899609-overview
- Vascular Rings, Pulmonary Slings, and Other Vascular Abnormalities. Diagnosis and Management of Adult Congenital Heart Disease (Third Edition) 2018, Pages 429-439 https://doi.org/10.1016/B978-0-7020-6929-1.00042-3
- McElhinney DB, Clark BJ 3rd, Weinberg PM, Kenton ML, McDonald-McGinn D, Driscoll DA, et al. Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branching. J Am Coll Cardiol. 2001 Jun 15. 37(8):2114-9.





{kind=link}