
Facial paralysis
Facial paralysis occurs when a person is no longer able to move some or all of the muscles on one or both sides of the face. The facial nerve (cranial nerve 7) that controls your facial muscles passes through a narrow corridor of bone on its way to your face. Facial weakness or paralysis may cause one corner of your mouth to droop, and you may have trouble retaining saliva on that side of your mouth. Facial paralysis may also make it difficult to close the eye on the affected side of your face. See your health care provider if you have weakness or numbness in your face. Seek emergency medical help right away if you have these symptoms along with a severe headache, seizure, or blindness.
Follow your health care provider’s instructions on how to take care of yourself at home. Take any medicines as directed.
If the eye cannot fully close, the cornea must be protected from drying out with prescription eye drops or gel.
Facial nerve anatomy
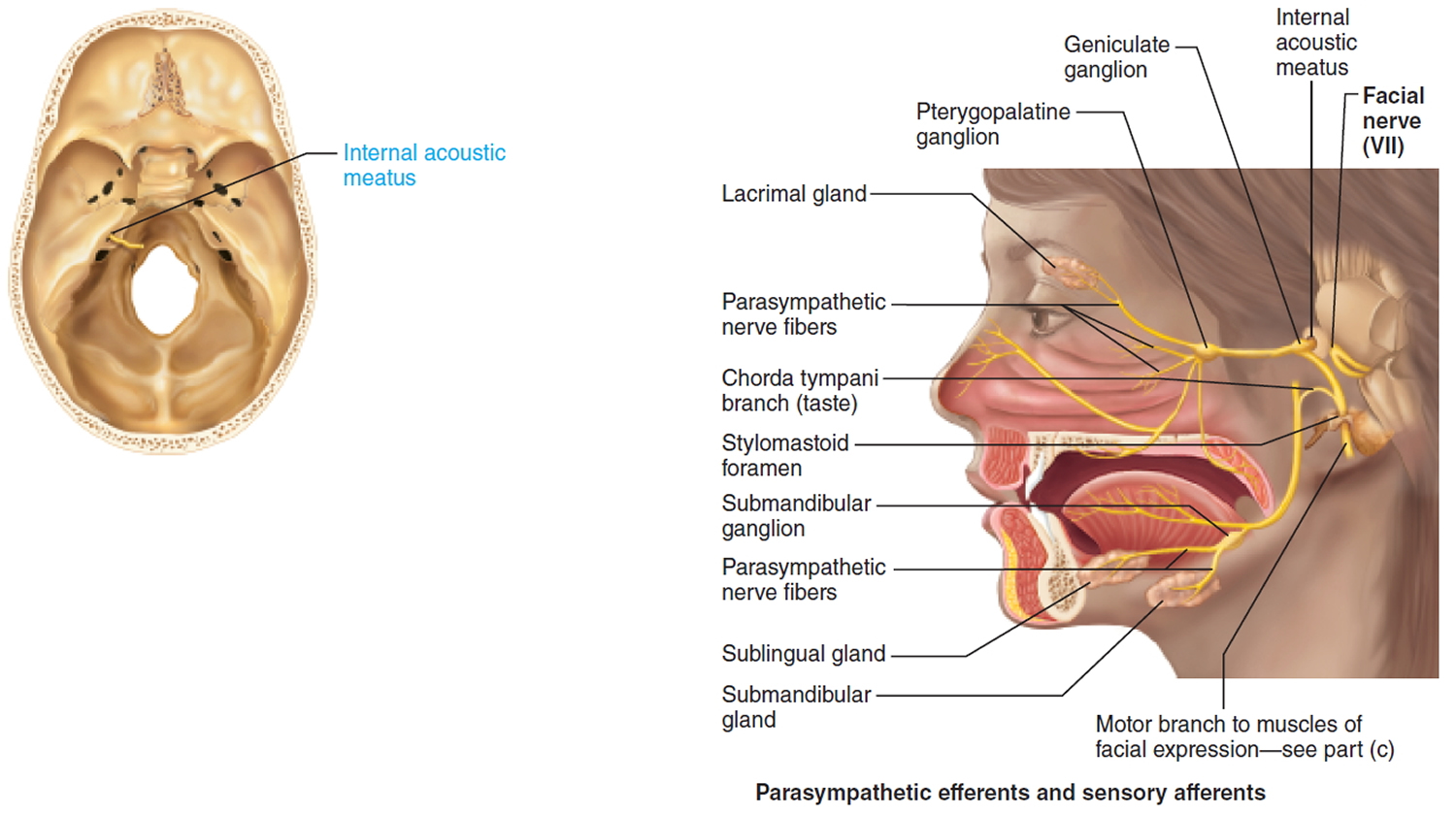
The facial nerve (cranial nerve 7) is a mixed nerve: Chief somatic motor nerve to the facial muscles; parasympathetic innervation to glands; special sensory taste from the tongue.
Sensory function: Special visceral sensory from taste buds on anterior two-thirds of tongue. General somatic sensory from small patch of skin on the ear.
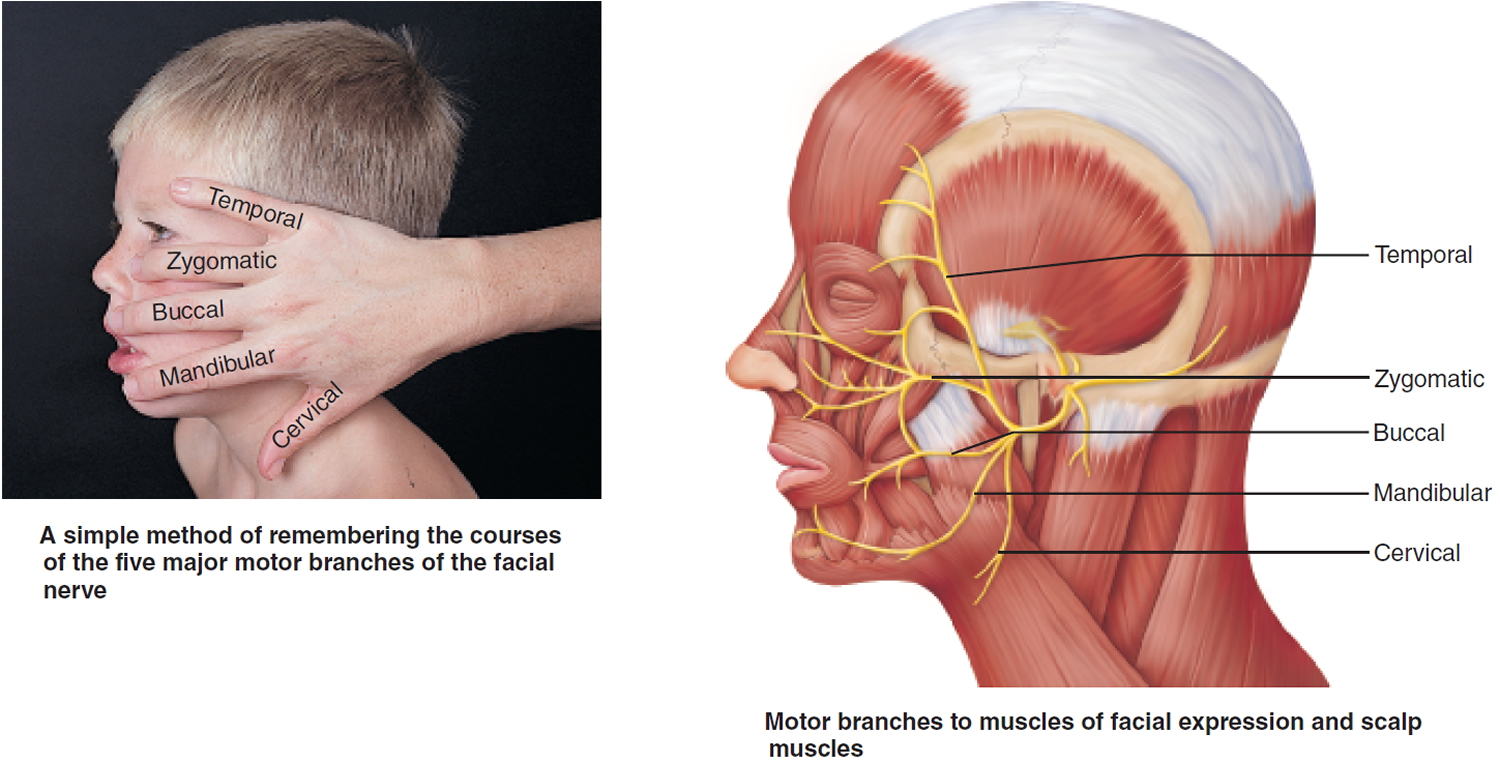
Somatic motor function: Five major branches on face: temporal, zygomatic, buccal, mandibular, and cervical, to innervate the facial muscles. Also innervates the posterior belly of digastric. Afferent proprioceptor fibers return from these muscles.
Visceral motor function (parasympathetic): Innervate the lacrimal (tear) glands, nasal and palatine glands, and the submandibular and sublingual salivary glands.
Effect of Damage: Bell’s palsy, characterized by paralysis of facial muscles on affected side and partial loss of taste sensation, may develop rapidly (often overnight). It is caused by herpes simplex (viral) infection, which produces inflammation and swelling of the facial nerve. The lower eyelid droops, the corner of the mouth sags (making it difficult to eat or speak normally), and the eye constantly drips tears and cannot be completely closed. The condition may disappear spontaneously without treatment.
Origin: Fibers emerge from the pons, just lateral to abducens.
Pathway: Fibers enter the temporal bone via the internal acoustic meatus. Chorda tympani branches off to innervate the two salivary glands and tongue. Branch to facial muscles emerges from the temporal bone through the stylomastoid foramen and courses to lateral aspect of face. Cell bodies of sensory neurons are in geniculate ganglion. Cell bodies of postganglionic parasympathetic neurons are in pterygopalatine and submandibular ganglia on the trigeminal nerve
Figure 1. Facial nerve (Cranial nerve 7)
Facial paralysis causes
Facial paralysis is almost always caused by:
- Damage or swelling of the facial nerve (seventh cranial nerve or CN VII), which carries signals from the brain to the muscles of the face. The facial nerve has both an intracranial, intratemporal, and extratemporal course as its branches. The facial nerve has a motor and parasympathetic function as well as taste to the anterior two-thirds of the tongue. The facial nerve (seventh cranial nerve or CN VII) also controls salivary and lacrimal glands. The motor function of the peripheral facial nerve controls the upper and lower facial muscles.
- Damage to the area of the brain that sends signals to the muscles of the face
Summary of causes of facial nerve palsy 1
- Birth
- Molding
- Forceps delivery
- Dystrophia myotonica
- Möbius syndrome (facial diplegia associated with other cranial nerve deficits)
- Trauma
- Basal skull fractures
- Facial injuries
- Penetrating injury to middle ear
- Altitude paralysis (barotrauma)
- Scuba diving (barotrauma)
- Lightning
- Neurologic
- Opercular syndrome (cortical lesion in facial motor area)
- Millard-Gubler syndrome (abducens palsy with contralateral hemiplegia caused by lesion in base of pons involving corticospinal tract)
- Infection
- External otitis
- Otitis media
- Mastoiditis
- Chickenpox
- Herpes zoster cephalicus (Ramsay Hunt syndrome)
- Encephalitis
- Poliomyelitis (type 1)
- Mumps
- Mononucleosis
- Leprosy
- Influenza
- Coxsackievirus
- Malaria
- Syphilis
- Scleroma
- Tuberculosis
- Botulism
- Acute hemorrhagic conjunctivitis (enterovirus 70)
- Gnathostomiasis
- Mucormycosis
- Lyme disease
- Cat scratch
- Acquired immunodeficiency syndrome (AIDS)
- Metabolic
- Diabetes mellitus
- Hyperthyroidism
- Pregnancy
- Hypertension
- Acute porphyria
- Vitamin A deficiency
- Neoplastic
- Benign lesions of parotid
- Cholesteatoma
- Seventh nerve tumor
- Glomus jugulare tumor
- Leukemia
- Meningioma
- Hemangioblastoma
- Sarcoma
- Carcinoma (invading or metastatic)
- Anomalous sigmoid sinus
- Carotid artery aneurysm
- Hemangioma of tympanum
- Hydradenoma (external canal)
- Facial nerve tumor (cylindroma)
- Schwannoma
- Teratoma
- Hand-Schüller-Christian disease
- Fibrous dysplasia
- Neurofibromatosis II
- Toxic
- Thalidomide (Miehlke syndrome, cranial nerves VI and VII with congenital malformed external ears and deafness)
- Ethylene glycol
- Alcoholism
- Arsenic intoxication
- Tetanus
- Diphtheria
- Carbon monoxide
- Iatrogenic
- Mandibular block anesthesia
- Antitetanus serum
- Vaccine treatment for rabies
- Postimmunization
- Parotid surgery
- Mastoid surgery
- Post-tonsillectomy and adenoidectomy
- Iontophoresis (local anesthesia)
- Embolization
- Dental
- Idiopathic
- Bell palsy
- Melkersson-Rosenthal syndrome (recurrent alternating facial palsy, furrowed tongue, faciolabial edema)
- Hereditary hypertrophic neuropathy (Charcot-Marie-Tooth disease, Dejerine-Sottas disease)
- Autoimmune syndrome
- Amyloidosis
- Temporal arteritis
- Thrombotic thrombocytopenic purpura
- Periarteritis nodosa
- Landry-Guillain-Barré syndrome (ascending paralysis)
- Multiple sclerosis
- Myasthenia gravis
- Sarcoidosis (Heerfordt syndrome, uveoparotid fever)
- Osteopetrosis
While there are many potential causes of facial paralysis, including idiopathic, traumatic, neoplastic, congenital, and autoimmune, about 70% of facial nerve palsies wind up with a diagnosis of Bell palsy 2.
In people who are otherwise healthy, facial paralysis is often due to Bell palsy. Bell palsy is the most common peripheral paralysis of the seventh cranial nerve (facial nerve) that has become inflamed with an onset that is rapid and unilateral. Bell palsy is more common in diabetics and in pregnant females. Bell’s palsy is by definition idiopathic in nature 2. Bell’s palsy is thought to result from compression of the seventh cranial nerve at the geniculate ganglion. The first portion of the facial canal, the labyrinthine segment is the narrowest and it is here that most cases of compression occur. Due to the narrow opening of the facial canal, inflammation causes compression and ischemia of the nerve. The most common finding is a unilateral facial weakness that includes the muscles of the forehead.
Stroke may cause facial paralysis. With a stroke, other muscles on one side of the body may also be involved.
Facial paralysis that is due to a brain tumor usually develops slowly. Symptoms can include headaches, seizures, or hearing loss.
In newborns, facial paralysis may be caused by trauma during birth.
Other causes include:
- Infection of the brain or surrounding tissues
- Lyme disease
- Sarcoidosis
- Tumor that presses on the facial nerve
Bell palsy
A most common entity of facial nerve paralysis is Bell palsy, which is unilateral and is considered to be of idiopathic etiology. The annual incidence of Bell palsy is approximately 15 to 20 per 100,000 with 40,000 new cases each year and the lifetime risk is 1 in 60 2. There is an 8% to 12% recurrence rate. Even without treatment, 70% of patients will have complete resolution. There is no gender or racial preference, and palsy can occur at any age, but more cases are seen in mid and late life with the median age of onset at 40 years. Risk factors include diabetes, pregnancy, preeclampsia, obesity, and hypertension 3.
A viral cause (ie, herpes simplex virus, varicella-zoster virus, and Epstein-Barr virus) has been suspected as a precursor inciting factor 4.
Bell palsy normally has a sudden onset that is often preceded by facial dysesthesia, epiphora, pain, hyperacusis, dysgeusia, and decreased function of the lacrimal gland 1.
Ramsay Hunt syndrome
Ramsay Hunt described a syndromic occurrence of facial paralysis, herpetiform vesicular eruptions, and vestibulocochlear dysfunction 5.
Patients presenting with Ramsay Hunt syndrome generally have a greater risk of hearing loss than do patients with Bell palsy, and the course of disease is more painful. Moreover, a lower recovery rate is observed in these patients 6.
Medical treatment is equivalent to that for Bell palsy; most often, a combination of steroids and antiviral agents is used 7.
Lyme disease
Infection with Borrelia burgdorferi via tick bites reveals another cause of facial paralysis, thereby presenting along with all the symptoms of Lyme disease. Of patients affected with Lyme disease, 10% develop facial paralysis, with 25% of these patients presenting with bilateral palsy 8.
Bacterial infection
Bacterial infection also may lead to facial nerve paralysis, most often correlated to acute otitis media or externa. Slow-onset facial nerve palsy is observed in patients with cholesteatoma.
Noninfectious causes
Noninfectious causes of facial nerve palsy include head trauma affecting the intracranial intratemporal course of the facial nerve or, less commonly, the infratemporal course, as seen in facial blunt or sharp injury 9.
Iatrogenic injury to the facial nerve most often is seen after cervicofacial rhytidectomies, surgery of the parotid gland, acoustic neuroma resection, or tumor resection at any point along the course of the facial nerve. Therefore, when facial paralysis occurs after surgery, operative exploration must follow if uncertainty exists concerning the intactness of the facial nerve. Due to topographic relations and/or tumor extension, the facial nerve occasionally must be sacrificed voluntarily as part of sound oncologic management.
Tumor of the facial nerve (eg, hemangioma, neuroma) or tumors in the direct vicinity of the facial nerve often are concomitant with facial nerve palsy. In general, gradual onset of paralysis may lead to suspicion of a tumor as the cause. However, several authors have demonstrated a sudden onset of facial nerve palsy in patients with tumors (20-27%) 10.
Facial paralysis symptoms
Bell’s palsy symptoms
Patients present with rapid and progressive symptoms over the course of a day to a week often reaching a peak in severity on 72 hours. Weakness will be partial or complete to one-half of the face, resulting in weakness of the eyebrows, forehead, and angle of the mouth. Patients may present with an inability to close the affected eyelid or lip on the affected side.
The key physical exam finding is a partial or complete weakness of the forehead. If forehead strength is preserved, a central cause should be investigated. Patients may also complain of a difference in taste, sensitivity to sound, otalgia, and changes to tearing and salivation.
Ocular features include:
- Corneal exposure
- Lagophthalmos
- Brow droop
- Paralytic ectropion of the lower lid
- Upper eyelid retraction
- Decreased tear output
- Loss of nasolabial fold
Facial paralysis diagnosis
Your health care provider will perform a physical exam and ask questions about your medical history and symptoms, including:
- Are both sides of your face affected?
- Have you recently been sick or injured?
- What other symptoms do you have? For example, drooling, excessive tears from one eye, headaches, seizures, vision problems, weakness, or paralysis.
Clinical diagnosis is based on 3 steps: (1) identification of the affected site, (2) underlying cause (trauma, infectious, neoplastic), and (3) clinical staging (eg, with use of the House-Brackmann scale).
Physical examination
A thorough head and neck examination is paramount, with occasional use of tests for salivation, tearing, and taste; these are the first steps in determining the site of injury. Physical examination findings reveal affected facial musculature movement.
Tests for facial innervation include the following:
- Forehead wrinkling (frontalis muscle)
- Eye closure (orbicularis oculi muscle)
- Wide smile
- Whistling
- Blowing (eg, buccinator muscle, orbicularis oris muscle, zygomatic muscle)
During the patient’s initial consultation, evaluate general muscle status (latissimus muscle, rectus abdominis muscle) for eventual reconstruction.
House-Brackmann scale
Clinically, injury to the infratemporal facial nerve can be classified by degree. Multiple classifications of facial nerve injury are found in the literature. The most frequently used is the House-Brackmann scale (see Table 1 below) 11.
The House-Brackmann Facial Nerve Grading System can be used to describe the degree of facial nerve weakness. House and Brackmann staged injury from grade 1-6 with different chances of spontaneous recovery, grade of 1 (no weakness) to 6 (complete weakness). These stages correspond with the pathologic findings of neurapraxia, axonotmesis, neurotmesis, and partial and complete transection of the facial nerve.
A clinical House-Brackmann grade 1 injury refers to neurapraxia, which is the most likely stage for spontaneous recovery.
Axonotmesis is the term for longer compression of the nerve, clinically a House-Brackmann level 2-3 injury, with temporary axonoplasmal flow interruption and subsequent Wallerian anterograde degeneration. Degeneration in axonotmesis is most often incomplete, with more or fewer axons surviving. Thus, partial facial weakness often results.
Neurotmesis is a state of permanent loss of axons further characterized by (partial) demyelinization leading to moderate to severe facial musculature dysfunction. Regenerative impulses may end in facial synkinetic movements, mass movements, or contracture.
Finally, clinical findings in House-Brackmann stage 5 and 6 injuries (partial or complete transection of the facial nerve) are either the retaining of minimal facial musculature movements or complete loss of function (grade 6).
Table 1. House-Brackmann Classification of Facial Function
| Grade | Characteristics |
| 1. Normal | Normal facial function in all areas |
| 2. Mild dysfunction | Gross Slight weakness noticeable on close inspection May have slight synkinesis At rest, normal symmetry and tone Motion Forehead – Moderate to good function Eye – Complete closure with minimal effort Mouth – Slight asymmetry |
| 3. Moderate dysfunction | Gross Obvious but not disfiguring difference between sides Noticeable (but not severe) synkinesis, contracture, or hemifacial spasm At rest, normal symmetry and tone Motion Forehead – Slight to moderate movement Eye – Complete closure with effort Mouth – Slightly weak with maximum effort |
| 4. Moderately severe dysfunction | Gross Obvious weakness and/or disfiguring asymmetry At rest, normal symmetry and tone Motion Forehead – None Eye – Incomplete closure Mouth – Asymmetrical with maximum effort |
| 5. Severe dysfunction | Gross Only barely perceptible motion At rest, asymmetry Motion Forehead – None Eye – Incomplete closure Mouth – Slight movement |
| 6. Total paralysis | No movement |
Tests that may be ordered include:
- Blood tests, including blood sugar, CBC, (ESR), Lyme test
- CT scan of the head
- Electromyography
- MRI of the head
Imaging studies
Computed tomography (CT) scanning and magnetic resonance imaging (MRI) are useful in the diagnosis of injury to intratemporal and/or intracranial affections of the facial nerve, as they may reveal temporal fracture patterns (vertical, transversal, mixed) and edema formation. Under certain circumstances, the facial nerve can be viewed, and swelling or disruption may be seen 12.
Electrophysiologic studies
Electrophysiology can be useful to determine the extent of nerve disruption, possible outcome, and treatment options 13. Most frequently, the minimal and maximal stimulation test (MST) and electroneuronography (ENog) are used. These tests are performed with percutaneous stimulation of the facial nerve.
Electroneuronography (ENog) studies are required to determine timing and necessity of surgical intervention (decompression or microneurorrhaphy) 14.
Electroneuronography (ENog) records a compound action potential, as well as latency after nerve stimulation. Degeneration of 90% or more has been shown to predict poor prognosis without surgical intervention 15.
A study by Azuma et al 16 indicated that electroneuronography (ENog) results can predict the development of facial synkinesis. The investigators reported that study patients who, 10-14 days following the onset of facial palsy, had an electroneuronography (ENog) value below 46.5%, were at increased risk of developing oral-ocular synkinesis 12 months after facial palsy first occurred.
Additional tests
For suspected intracranial or infratemporal injury, always perform a Schirmer test of tearing to assess lacrimal gland function.
Testing with different aromatic agents is needed to determine the integrity of afferent impulses from the anterior two thirds of the tongue.
Facial paralysis treatment
Facial paralysis treatment depends on the cause. Follow your health care provider’s treatment recommendations.
Your health care provider may refer you to a physical, speech, or occupational therapist. If facial paralysis from Bell palsy lasts for more than 6 to 12 months, plastic surgery may be recommended to help the eye close and improve the appearance of the face.
Botulinum toxin therapy
Management of synkinesis and hyperkinesis can include botulinum toxin (Botox) injection. This technique yields good results in the control of these sequelae of reinnervation procedures but must be repeated approximately every 3 months. Usually, 5-10 units are injected initially to control eyebrow spasm, and an additional 10-20 units are injected into the zygomaticus muscle and then repeated with an adapted dose as needed 17.
Bell’s palsy treatment
It is important to know that spontaneous recovery does occur and hence the role of treatment remains questionable 2.
Corticosteroids are the main treatment with a common regimen consisting of 60 mg to 80 mg a day for approximately 1 week. There is also some evidence stating corticosteroids and antivirals combined improved the outcome of Bell’s palsy compared with corticosteroids alone. A meta-analysis in 2009 found that steroids alone were the treatment of Bell’s palsy and the addition of antivirals did not meet statistical significance.
For patients with severe facial nerve palsy (House-Brackmann IV or greater) can be offered combination therapy with steroids and antivirals. There was no significant increase in adverse reactions from antivirals compared with either placebo or corticosteroids. Patients should be instructed to use eye lubrication and patch the affected eye at bedtime to reduce the likelihood of a corneal abrasion.
Surgical options can be considered when there is no improvement in symptoms after weeks or months. Techniques to present eye desiccation range from eyelid weights to muscle transfers. Facial nerve decompression has not been found to be a recommended treatment option and is considered on a case by case basis. Prior studies evaluating facial nerve compression have been of poor quality. It is recommended to refer to a specialist (plastic surgery, neurology, otolaryngology) sooner rather than later if no improvement has been seen in 4 weeks to explore more aggressive treatments 18.
Facial paralysis prognosis
In a study of 100 free muscle transfers (93 patients total), Terzis et al 19 demonstrated an overall improved result postoperatively in 94% of the patients, with 80% of patients being ranked as having a moderate or better result compared with the preoperative stage.
The investigators also found that women received higher scores and had an earlier onset of muscle function than men, younger patients had better results than older patients, and patients with a developmental cause of facial nerve paralysis had a better outcome than did patients with posttraumatic facial nerve paralysis. Intraoperative ischemia was not found to correlate with onset of muscle function.
Concerning outcome and donor muscle selection, patients in the study with pectoralis minor muscle transplants were found to have an earlier onset of muscle function than did those with gracilis transfers.
Overall, free tissue transfer to the face can be considered a safe and efficient method for the restoration of facial muscle movement.
References- May M, Klein SR. Differential diagnosis of facial nerve palsy. Otolaryngol Clin North Am. 1991 Jun. 24(3):613-45.
- Warner MJ, Hutchison J, Varacallo M. Bell Palsy. [Updated 2019 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482290
- Zhao H, Zhang X, Tang YD, Zhu J, Wang XH, Li ST. Bell’s Palsy: Clinical Analysis of 372 Cases and Review of Related Literature. Eur. Neurol. 2017;77(3-4):168-172.
- Schirm J, Mulkens PS. Bell’s palsy and herpes simplex virus. APMIS. 1997 Nov. 105(11):815-23.
- Hunt JR. On herpetiform inflammation of the geniculate ganglion: A new syndrome and its complications. Nerve Ment Dis. 1907. 34:73.
- Murakami S, Hato N, Horiuchi J, et al. [Clinical features and prognosis of facial palsy and hearing loss in patients with Ramsay Hunt syndrome]. Nippon Jibiinkoka Gakkai Kaiho. 1996 Dec. 99(12):1772-9.
- Niparko JK. The acute facial palsies. Jackler RK, ed. Neurotology. St. Louis: Mosby; 1994. 1311.
- Clark JR, Carlson RD, Sasaki CT, et al. Facial paralysis in Lyme disease. Laryngoscope. 1985 Nov. 95(11):1341-5.
- Thakar A, Gupta MP, Srivastava A, Agrawal D, Kumar A. Nonsurgical Treatment for Posttraumatic Complete Facial Nerve Paralysis. JAMA Otolaryngol Head Neck Surg. 2018 Apr 1. 144 (4):315-21.
- Jackson CG, Glasscock ME 3rd, Hughes G, Sismanis A. Facial paralysis of neoplastic origin: diagnosis and management. Laryngoscope. 1980 Oct. 90(10 Pt 1):1581-95.
- House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985 Apr. 93(2):146-7.
- Kumar A, Mafee MF, Mason T. Value of imaging in disorders of the facial nerve. Top Magn Reson Imaging. 2000 Feb. 11(1):38-51.
- Fisch U. Surgery for Bell’s palsy. Arch Otolaryngol. 1981 Jan. 107(1):1-11.
- Kumai Y, Ise M, Miyamaru S, Orita Y. Delayed transmastoid facial nerve decompression surgery in patients with Ramsay-Hunt syndrome presenting with neurophysiologically complete paralysis. Acta Otolaryngol. 2018 May 15. 1-5.
- Ruboyianes J, Adour KK, Santos D, et al. The maximal stimulation and facial nerve conduction latency tests: Predicting the outcome of Bell’s palsy. Laryngoscope. 1994. 104(suppl):1-6.
- Azuma T, Nakamura K, Takahashi M, et al. Electroneurography in the acute stage of facial palsy as a predictive factor for the development of facial synkinesis sequela. Auris Nasus Larynx. 2018 Aug. 45 (4):728-31.
- Elston JS. The management of blepharospasm and hemifacial spasm. J Neurol. 1992 Jan. 239(1):5-8.
- Tseng CC, Hu LY, Liu ME, Yang AC, Shen CC, Tsai SJ. Bidirectional association between Bell’s palsy and anxiety disorders: A nationwide population-based retrospective cohort study. J Affect Disord. 2017 Jun;215:269-273.
- Terzis JK, Noah ME. Analysis of 100 cases of free-muscle transplantation for facial paralysis. Plast Reconstr Surg. 1997 Jun. 99(7):1905-21.





{kind=link}