
Fibromatosis colli
Fibromatosis colli also called congenital muscular torticollis, sternocleidomastoid tumor or pseudotumor of the sternocleidomastoid muscle of infancy, is a rare benign tumor of the sternocleidomastoid muscle consisting of fibroblastic proliferation seen in infancy 1. Fibromatosis colli of infancy is classified in the category of benign fibroblast proliferations as classified by the World health organization in 2002 of soft tissue tumors 2. Fibromatosis colli is seen in newborn after difficult, prolonged labor, assisted delivery, and breech deliveries 3. Fibromatosis colli is a self limiting lesion, presents as a firm to hard, immobile, fusiform swelling in the lower or middle portion of the sternocleidomastoid muscle and usually appears within the first few weeks of life. Fibromatosis colli lesion typically appears 10-14 days after birth 4. Most of the cases present with torticollis but there are exceptions.
The reported prevalence is 0.4%, and it affects boys more than girls 5. Fibromatosis colli is more common on the right side of the neck, is usually unilateral, and classically manifests as a firm, non-tender neck swelling that develops during the first four weeks of life 6. Fibromatosis colli is associated with torticollis in approximately 20% of cases, and is the most common cause of congenital muscular torticollis 7.
Fibromatosis colli differential diagnosis includes congenital lesions such as branchial cyst, thyroglossal cyst, inflammatory lesions like tuberculous lymphadenitis and neoplastic conditions which could be benign (haemangioma, cystic hygroma) or malignant (neuroblastoma, rhabdomyosarcoma and lymphoma) 8.
Fibromatosis colli of infancy is a self-limiting condition and usually resolves within 4-8 months 9 and requires no more than physiotherapy. As the treatment of fibromatosis colli is usually conservative and avoids surgical procedures by employing physiotherapy, the diagnostic, noninvasive technique of fine-needle aspiration cytology (FNAC) becomes important. Fibromatosis colli has to be differentiated from congenital lesions, inflammatory lesions, and neoplastic conditions—both benign and malignant—that may occur at that site 10. Fine-needle aspiration cytology is a simple technique that will help in excluding the above conditions and also in avoiding surgical procedures. Cytologic smears show non-specific findings such as spindle cells, degenerating muscle fibers and multinucleate giant cells 1. Fibromatosis colli can be differentiated from other forms of infantile fibromatosis on the basis of the clinical features such as age, site, infiltrative pattern, and cytological features such as bland-appearing fibroblasts, degenerative, atrophic skeletal muscle, and muscle giant cells without inflammatory cells in a clean background 11. In contrast to other forms of fibromatosis, a noninvasive, conservative management is usually the line of treatment for fibromatosis colli in most of the cases.
Fibromatosis colli in newborn key points
- Fibromatosis colli is an unusual cause of a neck lump in infants, but the most common cause of congenital muscular torticollis.
- Diagnosis can be made confidently with a clinical examination and ultrasonography, allowing early parental reassurance and avoiding invasive investigations.
- The mainstay of treatment is physiotherapy, and results in resolution in the majority of cases.
Figure 1. Sternocleidomastoid muscle
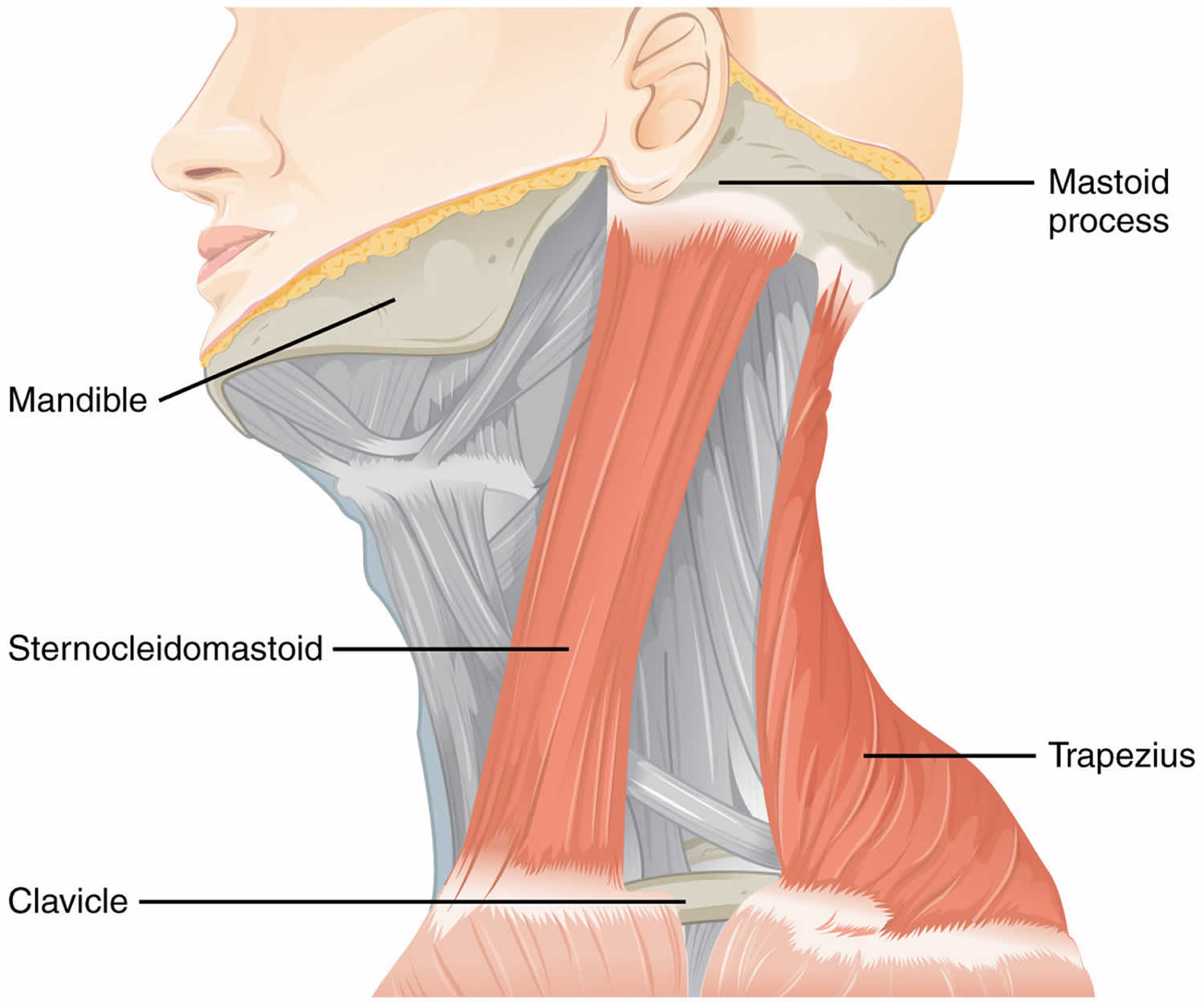
Figure 2. Fibromatosis colli in newborn

Figure 3. Fibromatosis colli ultrasound
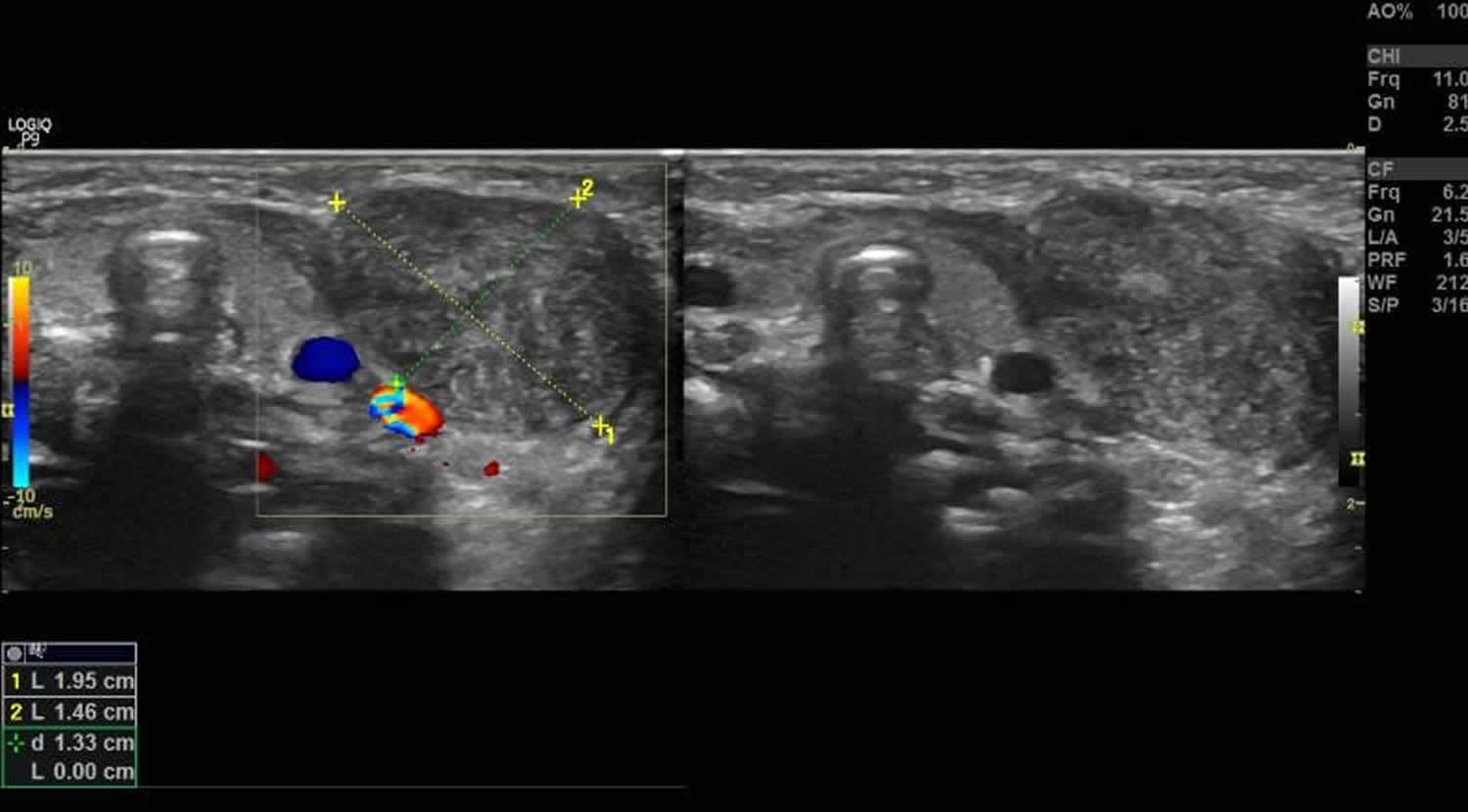
Footnote: Fibromatosis colli ultrasound showed a thickened sternocleidomastoid muscle on the left side; it had a fusiform appearance and heterogenous echotexture. The fibrillar structure of the muscle fibers was, however, maintained. The right sternocleidomastoid muscle appeared normal. There was no cervical lymphadenopathy.
[Source 12 ]Fibromatosis colli in adults
Fibromatosis colli in adults is quite rare 13, although it is the third most common congenital deformity in the newborn 14. When left untreated at an early age, deficits in lateral and rotational range of motion can occur along with irreversible facial and skeletal deformities that develop over time. Subtle cases can go unnoticed until early adulthood, with predominant fibrotic replacement in the sternocleidomastoid muscle making physical therapy and chemodenervation mostly ineffective 13. Surgical treatment of neglected fibromatosis colli in adults can be difficult due to adjacent tissue contractures, adhesions, and extensive fibrosis 15. Surgical intervention, in these cases, can prove effective in alleviating pain, improving function and cosmesis 16.
Figure 4. Fibromatosis colli in adults
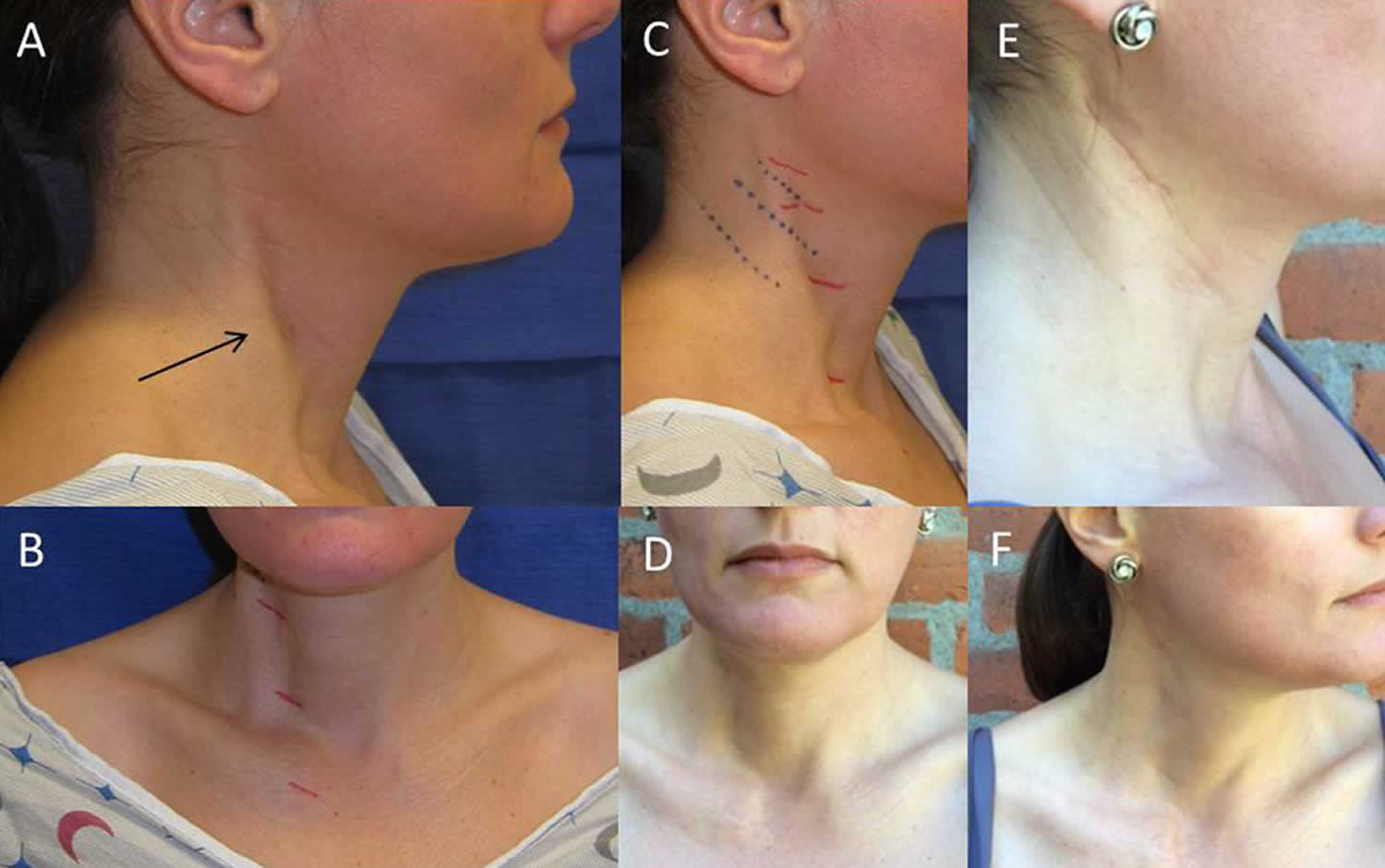
Footnote:A 42-year old woman, who noticed right head tilt and bilateral shoulder pain in her late twenties, had previously undergone resection of the anterior belly of the right sternocleidomastoid muscle 5 years ago after failed physical therapy and Botox injections. Images of tethering and anterior sternocleidomastoid muscle defect pre-operatively and post-operative resolution of marked tethering and appearance of incision. Noticeable tethering from the lateral view marked with an arrow (A) and from the anterior view with previous stair-step incision marked in red (B). Lateral view of pre-operative planning for Z-plasty incision with Langer lines indicated in blue (C). Two views of post-operative decrease in tethering (D,F). Post-operative appearance of Z-plasty incision at 6 months (E).
[Source 13 ]Fibromatosis colli causes
The exact causes of fibromatosis colli are not yet known. Although the pathogenesis is unclear, there is an association between fibromatosis colli and birth injury such as breech delivery, instrumental delivery and difficult labor, which is otherwise debatable as some of the cases do not have any history of birth injury 17. It has been postulated that in a difficult delivery, compression of the neck can cause ischaemic injury or venous occlusion, leading to damaged muscle fibers that then fibrose 7. Another proposed mechanism is tearing of the sternocleidomastoid muscle during delivery resulting in a hematoma, ultimately causing atrophy of muscle fibers 18. When these lesions are biopsied, the most common feature on cytology is thin, spindle-shaped fibroblasts 19, 6.
Fibromatosis colli signs and symptoms
Fibromatosis colli presentation is usually with torticollis with restricted neck’s movements for the newborn and a neck mass and is most frequently related to birth trauma (e.g. forceps delivery and difficult labor) or malposition (e.g. breech) in the womb. On clinical examination, there may be a growing, hard neck mass 20.
Fibromatosis colli complications
fibromatosis colli complications include 21:
- plagiocephaly
- facial asymmetry
- scoliosis
- permanent loss of neck mobility.
Fibromatosis colli diagnosis
Ultrasonography is the preferred imaging modality, with a sensitivity of 100%. Ultrasonography is non-invasive, inexpensive and accessible 21. Features include a fusiform enlargement of the sternocleidomastoid muscle, generally in the lower two-thirds, with defined margins. Echogenicity varies, with 49% of masses being hyperechoic 7. Ultrasonography is also useful in excluding conditions considered in the differential diagnosis.
If further imaging is required to delineate the diagnosis, computed tomography (CT) or magnetic resonance imaging (MRI) can be used. CT images show isodense enlargement of the muscle, and on MRI there is increased signal intensity on T1 when compared with T2 weighted images, demonstrating the presence of fibrous tissue 18. MRI can also provide information on the surrounding fascial planes, relationship to vascular structures and airway, and bony involvement 7.
Fine needle aspiration for cytological investigation can be used to confirm diagnosis in a non-classical presentation. It is minimally invasive and can be used to avoid a more invasive procedure such as an excisional biopsy 6.
Fibromatosis colli treatment
Management is conservative and primarily involves physiotherapy with gentle, passive stretching exercise programs 18. Lee et al 22 suggested a protocol of 15 manual stretches of the muscle sustained for one second, and 10 seconds between stretches, for three repetitions. This was performed three times per week. Active positioning at home can also be suggested, where parents are taught to encourage the infant to sleep with their head turned to the affected side 23. When commenced within four months of the onset of symptoms, resolution should occur within three to four months and in 90% of patients 21.
For refractory cases, surgical tenotomy is an option. Botulinum toxin is currently being explored as an alternative treatment for children with ongoing symptoms despite physiotherapy, but further evidence of safety and long-term sequelae is required before this is accepted as a suitable treatment 21.
Fibromatosis colli prognosis
Infantile fibromatosis colli is a self-limiting condition and usually resolves within 4-8 months 9.
References- Kumar P, Sharma S, Kapil V. Fibromatosis colli: A rare cause of neck mass with cytological soft pointers. Cytopathology. 2019 Sep;30(5):549-551. https://doi.org/10.1111/cyt.12692
- Fletcher CD, Unni KK, Mertens F (2002) Fibromatosiscolli. In: World Health Organization classification of tumors: pathology and genetics of tumors of soft tissue and bone. IARC Press Publisher, France
- Rajalakshmi V, Selvambigai G, Jaiganesh. Cytomorphology of fibromatosis colli. J Cytol. 2009;26(1):41-42. doi:10.4103/0970-9371.54869 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3167991
- Fibromatosis colli of infancy: CT and sonographic findings. American Journal of Roentgenology. 1988;151: 1183-1184. 10.2214/ajr.151.6.1183 https://www.ajronline.org/doi/pdf/10.2214/ajr.151.6.1183
- Oliveira JC, Abreu MS, Gomes FM. Sternocleidomastoid tumour in neonate: Fibromatosis colli. BMJ Case Rep 2018. doi: 10.1136/bcr-2017-223543
- Baisakh MR, Mishra M, Narayanan R, Mohanty R. Cytodiagnosis of sternocleidomastoid tumor of infancy. J Cytol 2012;29(2):149–51. doi: 10.4103/0970-9371.97164
- Ablin DS, Jain K, Howell L, West DC. Ultrasound and MR imaging of fibromatosis colli (sternomastoid tumor of infancy). Pediatr Radiol 1998;28(4):230–33. doi: 10.1007/s002470050337
- Khan S, Jetley S, Jairajpuri Z, Husain M. Fibromatosis colli – a rare cytological diagnosis in infantile neck swellings. J Clin Diagn Res. 2014;8(11):FD08-FD9. doi:10.7860/JCDR/2014/10840.5154 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4290252
- Crawford SC, Harnsberger HR, Johnson L, Aoki JR, Giley J. Fibromatosis colli of infancy: CT and sonographic findings. AJR Am J Roentgenol. 1988 Dec;151(6):1183-4. doi: 10.2214/ajr.151.6.1183
- Sharma S, Mishra K, Khanna G. Fibromatosis Colli in infants: A cytologic study of eight cases. Acta Cytol. 2003;47:359–62.
- Akerman M. Soft tissues. In: Orell SR, Sterrett GF, Whitaker D, editors. Fine needle aspiration cytology. 4th ed. Philadelphia: Elsevier Churchill Livingstone; 2005. p. 414.
- Fibromatosis colli. https://radiopaedia.org/cases/fibromatosis-colli-11
- Uluer MC, Bojovic B. A Rare Cervical Dystonia Mimic in Adults: Congenital Muscular Torticollis (Fibromatosis colli), a Follow-up. Front Neurol. 2016;7:7. Published 2016 Feb 1. doi:10.3389/fneur.2016.00007 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4738269
- Do TT. Congenital muscular torticollis: current concepts and review of treatment. Curr Opin Pediatr (2006) 18(1):26–9.10.1097/01.mop.0000192520.48411.fa
- Oh I, Nowacek CJ. Surgical release of congenital torticollis in adults. Clin Orthop Relat Res (1978) 131:141–5.
- Lim KS, Shim JS, Lee YS. Is sternocleidomastoid muscle release effective in adults with neglected congenital muscular torticollis? Clin Orthop Relat Res (2014) 472(4):1271–8.10.1007/s11999-013-3388-6
- Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft tissue tumors. 4th ed. St Louis: Mosby; 2001. Fibrous tumors of infancy and childhood; pp. 273–5.
- Skelton E, Howlett D. Fibromatosis colli: The sternocleidomastoid pseudotumour of infancy. J Paediatr Child Health 2014;50(10):833–35. doi: 10.1111/jpc.12506
- Khalid S, Zaheer S, Wahab S, Siddiqui MA, Redhu N, Yusuf F. Fibromatosis colli: A case report. Oman Med J 2012;27(6):e011. doi: 10.5001/omj.2012.126
- Passarello L, Bhurawala H. Fibromatosis colli: An infant with neck swelling. Aust J Gen Pract. 2019 Nov;48(11):751-752. doi: 10.31128/AJGP-11-18-4770.
- Tempark T, Chatproedprai S, Mahayosnond A, Wananukul S. Fibromatosis colli, overlooked cause of neonatal torticollis. Int J Pediatr Otorhinolaryngol 2012;7(1):15–17. doi: 10.1016/j.pedex.2011.07.007
- Lee Y-T, Yoon K, Kim Y-B, et al. Clinical features and outcome of physiotherapy in early presenting congenital muscular torticollis with severe fibrosis on ultrasonography: A prospective study. J Pediatr Surg 2011;46(8):1526–31. doi: 10.1016/j.jpedsurg.2011.02.040
- Cheng JCY, Tang SP, Chen TMK. Sternocleidomastoid pseudotumor and congenital muscular torticollis in infants: A prospective study of 510 cases. J Pediatr 1999;134(6):712–16. doi: 10.1016/S0022-3476(99)70286-6





{kind=link}