
What are nitrates in urine
Nitrite and leucocyte esterase are indicators of urinary tract infection. Some bacteria, for example, Enterobacteriaceae, convert nitrates to nitrites.
Leukocyte esterase
Leukocyte esterase is an enzyme present in most white blood cells. A few white blood cells are normally present in urine and usually give a negative chemical test result. When the number of white blood cells in urine increases significantly, the urine screening test will become positive. Leukocyte esterase identifies the presence of white blood cells in the urine. The white blood cells release the Leukocyte esterase, presumably in response to bacteria in the urine. This is why leukocyte esterase is a subsequent test with a specificity of only 55% for urinary tract infection. Leukocyte esterase is good at detecting white blood cells in the urine, but white blood cells can be in the bladder for other reasons, like inflammatory disorders. Results of the urine screening test will be considered along with a microscopic examination for white blood cells in the urine.
When the urine screening is positive and/or the white blood cell count in urine is high, it may indicate that there is inflammation in the urinary tract or kidneys. The most common cause for white blood cells in urine (leukocyturia) is a bacterial urinary tract infection (UTI), such as a bladder or kidney infection. In addition to white blood cells, bacteria and red blood cells may also be seen in the microscopic examination. If bacteria are present, the chemical test for nitrite may also be positive.
Nitrite
The most accurate dipstick test is the nitrite test because bacteria must be present in the urine to convert nitrates to nitrites. The urine screening test detects nitrite and is based upon the fact that many bacteria can convert nitrate (a normal substance in urine) to nitrite. Normally, the urinary tract and urine are free of bacteria and nitrite. When bacteria enter the urinary tract, they can cause a urinary tract infection. A positive nitrite test result can indicate a urinary tract infection (UTI). However, several bacteria do not convert the nitrates to nitrites (such as those involving Enterococcus, Pseudomonas, and Acinetobacter) are not capable of converting nitrate to nitrite, someone can still have a urinary tract infection (UTI) despite a negative nitrite test, but those are usually involved in complicated urinary tract infections. The results of urine nitrite test will be considered along with the leukocyte esterase (above) and a microscopic urine examination.
The urine nitrite test takes 6 hours. This is why doctors request the first-morning urine, particularly in males. The specificity of the urine nitrite test is greater than 90%. This is direct confirmation of bacteria in the urine, which is urinary tract infection (UTI) by definition in patients with symptoms.
The presence of blood in urine (hematuria) can be helpful because bacterial infection of the transitional cell lining of the bladder can cause bleeding. This helps distinguish urinary tract infection from vaginitis and urethritis which do not cause blood in the urine.
In many labs, the presence of nitrites or leukocyte esterase will automatically trigger a microscopic evaluation of the urine for bacteria, white blood cells, and red blood cells. On microscopy, there should be no bacteria in uninfected urine, so any bacteria on a gram-stained urine under microscopy is highly correlated to urinary tract infection. A good urine sample with greater than 5 to 10 white blood cell/high powered field under microscopy is abnormal and highly suggestive of urinary tract infection in symptomatic patients.
Urine cultures are not needed in uncomplicated urinary tract infection. Urine should be cultured in all men and patients with diabetes mellitus, who are immunosuppressed, and women who are pregnant. Classic teaching on urine culture sets the gold standard for infected urine at greater than 10 colony forming units (CFU). Recent literature states that a patient who presents with symptoms and greater than 10 colony forming units (CFU) is diagnostic of infection. Urine cultures rarely help in the emergency department, except with recurrent urinary tract infection.
Urine is produced by the kidneys and the kidneys filter wastes out of the blood, help regulate the amount of water in the body, and conserve proteins, electrolytes, and other compounds that the body can reuse. Anything that is not needed is eliminated in the urine, traveling from the kidneys through ureters to the bladder and then through the urethra and out of the body. Urine is generally yellow and relatively clear, but each time a person urinates, the color, quantity, concentration, and content of the urine will be slightly different because of varying constituents.
Many disorders may be detected in their early stages by identifying substances that are not normally present in the urine and/or by measuring abnormal levels of certain substances. Some examples include glucose, protein, bilirubin, red blood cells, white blood cells, crystals, and bacteria. They may be present because:
- There is an elevated level of the substance in the blood and the body responds by trying to eliminate the excess in the urine.
- Kidney disease is present.
- There is a urinary tract infection present, as in the case of bacteria and white blood cells.
A complete urinalysis consists of three distinct testing phases:
- Visual examination, which evaluates the urine’s color and clarity
- Chemical examination, which tests chemically for about 9 substances that provide valuable information about health and disease and determines the concentration of the urine
- Microscopic examination, which identifies and counts the type of cells, casts, crystals, and other components such as bacteria and mucus that can be present in urine
A microscopic examination is typically performed when there is an abnormal finding on the visual or chemical examination, or if a healthcare practitioner specifically orders it.
Abnormal findings on a urinalysis may prompt repeat testing to see if the results are still abnormal and/or may be followed by additional urine and blood tests to help establish a diagnosis.
What is the correct technique for collecting urine sample for testing?
One to two ounces of urine is collected in a clean container. A sufficient sample is required for accurate results.
Urine for a urinalysis can be collected at any time. In some cases, a first morning sample may be requested because it is more concentrated and more likely to detect abnormalities.
Sometimes, you may be asked to collect a “clean-catch” urine sample. For this, it is important to clean the genital area before collecting the urine. Bacteria and cells from the surrounding skin can contaminate the sample and interfere with the interpretation of test results. With women, menstrual blood and vaginal secretions can also be a source of contamination. Women should spread the labia of the vagina and clean from front to back; men should wipe the tip of the penis. Start to urinate, let some urine fall into the toilet, then collect one to two ounces of urine in the container provided, then void the rest into the toilet.
A urine sample will only be useful for a urinalysis if taken to the healthcare provider’s office or laboratory for processing within a short period of time. If it will be longer than an hour between collection and transport time, then the urine should be refrigerated or a preservative may be added.
There are many factors that can affect or interfere with the tests that comprise a urinalysis. If instructed to do so, it is important to follow the directions carefully for a “clean-catch” sample. Give a complete history to your healthcare practitioner, including any prescribed or over-the-counter medications or supplements you may be taking. If you are a women, be sure to tell your healthcare practitioner whether you are menstruating.
Can a urinalysis be done in my healthcare practitioner’s office?
Many healthcare providers’ offices and clinics can perform the visual and chemical examinations of urine. Some may also be able to provide microscopic examinations. Sometimes, if abnormal results are found on the visual or chemical exams, your urine sample may be sent to a laboratory for the microscopic exam. Alternatively, your sample may be sent to a laboratory for a full urinalysis.
Are there home test kits available to test my urine?
Kits to perform a full urinalysis are not available because the test requires special equipment and technical skills. However, some commercial testing strips can be purchased at a pharmacy to perform part of the chemical examination, such as urine pH, urine glucose, and urine ketones.
How is urine test used?
The urinalysis is a set of screening tests that can detect some common diseases. It may be used to screen for and/or help diagnose conditions such as a urinary tract infections, kidney disorders, liver problems, diabetes or other metabolic conditions, to name a few.
A urinalysis is comprised of several chemical, microscopic and visual examinations used to detect cells, cell fragments and substances such as crystals or casts in the urine associated with the various conditions listed above. It can detect abnormalities that might require follow-up investigation and additional testing. Often, substances such as protein or glucose will begin to appear in the urine before people are aware that they may have a problem.
In people diagnosed with diseases or conditions, such as kidney disease or diabetes, the urinalysis may be used in conjunction with other tests, such as urine albumin, to follow treatment.
When is urine test ordered?
A urinalysis may sometimes be ordered when a person has a routine wellness exam, is admitted to the hospital, or will undergo surgery, or when a woman has a pregnancy checkup.
A urinalysis will likely be ordered when a person sees a healthcare practitioner complaining of symptoms of a urinary tract infection or other urinary system problem, such as kidney disease. Some signs and symptoms may include:
- Abdominal pain
- Back pain
- Painful or frequent urination
- Blood in the urine
Testing may also be ordered at regular intervals when monitoring certain conditions over time.
What does abnormal urine test result mean?
Urinalysis results can have many interpretations. Abnormal findings are a warning that something may be wrong and should be evaluated further. A healthcare practitioner must correlate the urinalysis results with a person’s symptoms and clinical findings and search for the causes of abnormal findings with other targeted tests, such as a comprehensive metabolic panel, complete blood count (CBC), renal panel, liver panel, or urine culture (for urinary tract infection).
Generally, the greater the concentration of the atypical substance, such as greatly increased amounts of glucose, protein, white blood cells (leuocytes) or red blood cells (erythrocytes), the more likely it is that there is a problem that needs to be addressed. However, the results do not tell the healthcare practitioner exactly what the cause of the finding is or whether it is a temporary or chronic condition.
A normal urinalysis does not guarantee that there is no illness. Some people will not release elevated amounts of a substance early in a disease process, and some will release them sporadically during the day, which means that they may be missed by a single urine sample. In very dilute urine, small quantities of chemicals may be undetectable.
For additional details on what specific results may mean, see the sections below on:
- Visual examination
- Chemical examination
- Microscopic examination
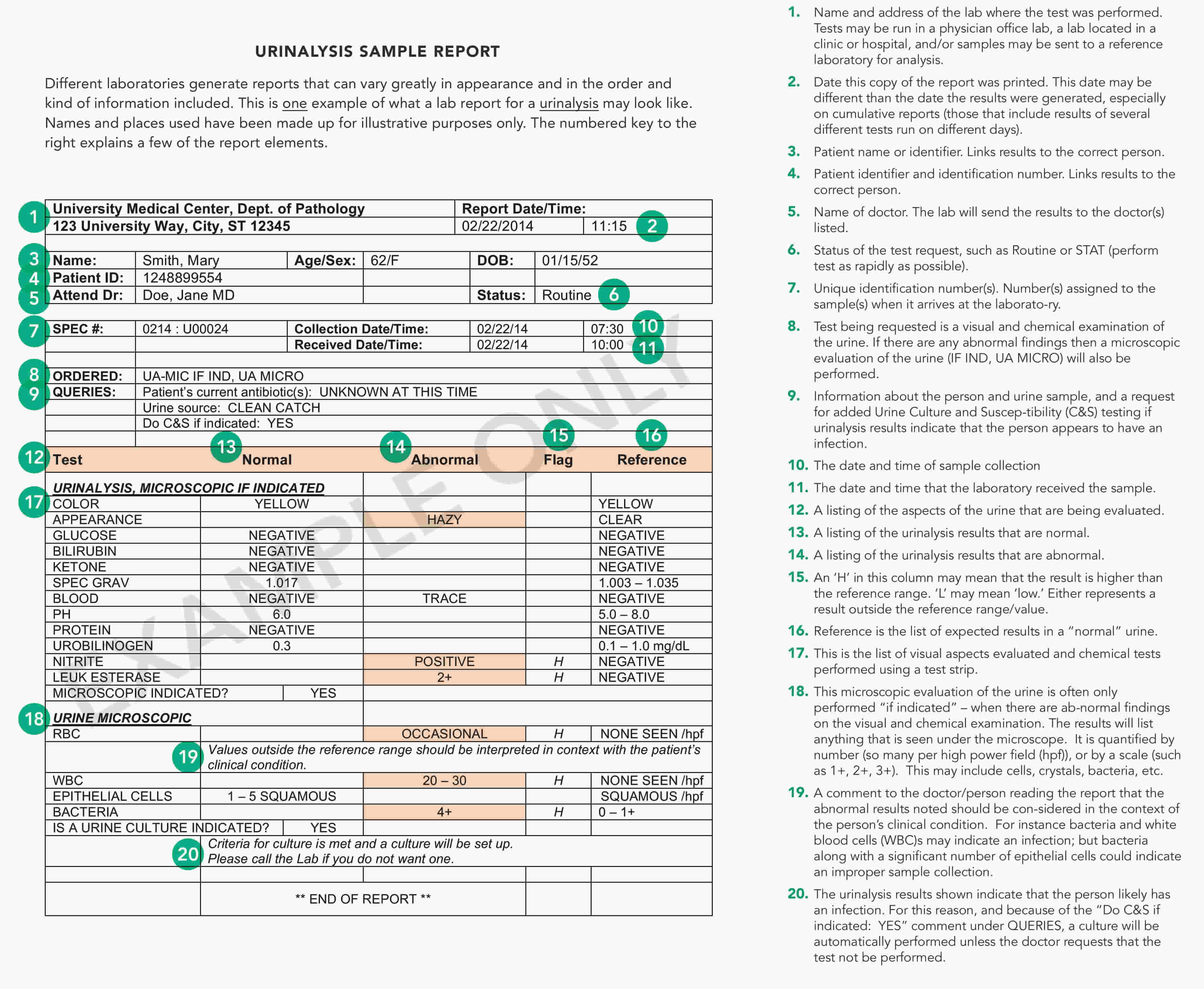
To see an example of a urinalysis lab report, see this sample report.
Figure 1. Urinalysis sample lab report
Visual examination
During the visual examination of the urine, the laboratory scientist observes the urine’s color and clarity. These can be signs of what substances may be present in the urine. They are interpreted in conjunction with results obtained during the chemical and microscopic examinations to confirm what substances are present. (See The Chemical Examination and The Microscopic Examination for details).
Urine color
Urine can be a variety of colors, most often shades of yellow, from very pale or colorless to very dark or amber. Unusual or abnormal urine colors can be the result of a disease process, several medications (e.g., multivitamins can turn urine bright yellow), or the result of eating certain foods. For example, some people can have red-colored urine after eating beets; the color is from the natural pigment of beets and is not a cause for worry. However, red-colored urine can also occur when blood is present in the urine and can be an indicator of disease or damage to some part of the urinary system. Another example is yellow-brown or greenish-brown urine that may be a sign of bilirubin in the urine (see The Chemical Examination section).
Urine clarity
Urine clarity refers to how clear the urine is. Usually, laboratorians report the clarity of the urine using one of the following terms: clear, slightly cloudy, cloudy, or turbid. “Normal” urine can be clear or cloudy. Substances that cause cloudiness but that are not considered unhealthy include mucus, sperm and prostatic fluid, cells from the skin, normal urine crystals, and contaminants such as body lotions and powders. Other substances that can make urine cloudy, like red blood cells, white blood cells, or bacteria, indicate a condition that requires attention.
Chemical examination
To perform the chemical examination, most clinical laboratories use commercially prepared test strips with test pads that have chemicals impregnated into them. The laboratory scientist dips the strip into urine, chemical reactions change the colors of the pads within seconds to minutes, and the laboratory scientist determines the result for each test. To reduce timing errors and eliminate variations in color interpretation, automated instruments are frequently used to “read” the results of the test strip.
The degree of color change on a test pad can give an estimate of the amount of substance present. For example, a slight color change in the test pad for protein may indicate a small amount of protein present in the urine whereas a deep color change may indicate a large amount.
The chemical examination is often done in conjunction with or may be followed by a microscopic examination of the urine if there are any abnormal results. Results from both sets of tests are then considered together for interpretation. Abnormal findings may be followed by additional urine and/or blood tests.
The most frequently performed chemical tests using reagent test strips are described below.
Specific gravity
Urine specific gravity is a measure of urine concentration. This test simply indicates how concentrated the urine is. Specific gravity measurements are a comparison of the amount of substances dissolved in urine as compared to pure water. If there were no substances present, the specific gravity of the urine would be 1.000 (the same as pure water). Since all urine has some substances in it, a urine specific gravity of 1.000 is not possible. If a person drinks excessive quantities of water in a short period of time or gets an intravenous (IV) infusion of large volumes of fluid, then the urine specific gravity may be very close to that of water. The upper limit of the test pad, a specific gravity of 1.035, indicates concentrated urine, one with many substances in a limited amount of water.
Knowing the urine concentration helps healthcare practitioners understand whether a urine specimen they are evaluating is the best one to detect a particular substance. For example, if they are looking for very small amounts of protein, a concentrated morning urine specimen would be the best sample.
pH
As with specific gravity, there are typical but not “abnormal” urine pH values. The urine is usually slightly acidic, about pH 6, but can range from 4.5-8. The kidneys play an important role in maintaining the acid-base balance of the body. Therefore, any condition that produces acids or bases in the body, such as acidosis or alkalosis, or the ingestion of acidic or basic foods can directly affect urine pH.
Some of the substances dissolved in urine will precipitate out to form crystals when the urine is acidic; others will form crystals when the urine is basic. If crystals form while the urine is being produced in the kidneys, a kidney stone or “calculus” can develop. By modifying urine pH through diet or medications, the formation of these crystals can be reduced or eliminated.
Bilirubin
This test screens for bilirubin in the urine. Bilirubin is not present in the urine of normal, healthy individuals. It is a waste product that is produced by the liver from the hemoglobin of red blood cells that are broken down and removed from circulation. It becomes a component of bile, a fluid that is released into the intestines to aid in food digestion.
In certain liver diseases, such as biliary obstruction or hepatitis, excess bilirubin can build up in the blood and is eliminated in urine. The presence of bilirubin in urine is an early indicator of liver disease and can occur before clinical symptoms such as jaundice develop.
The results of this test will be considered along with the result of urobilinogen (below). If positive, the healthcare practitioner will likely follow up with other laboratory tests, such as a liver panel, to help establish a diagnosis.
Urobilinogen
This test screens for urobilinogen in the urine. The results are considered along with those for urine bilirubin (above).
Urobilinogen is normally present in urine in low concentrations. It is formed in the intestine from bilirubin, and a portion of it is absorbed back into the blood. Positive test results may indicate liver diseases such as viral hepatitis, cirrhosis, liver damage due to drugs or toxic substances, or conditions associated with increased red blood cell destruction (hemolytic anemia). When urine urobilinogen is low or absent in a person with urine bilirubin and/or signs of liver dysfunction, it can indicate the presence of hepatic or biliary obstruction.
Protein
The protein test pad provides a rough estimate of the amount of albumin in the urine. Albumin makes up about 60% of the total protein in the blood. Normally, there will be no protein or a small amount of protein in the urine. When urine protein is elevated, a person has a condition called proteinuria.
Proteinuria may occasionally be seen in healthy individuals. Healthy people can have temporary or persistent proteinuria due to stress, exercise, fever, aspirin therapy, or exposure to cold, for example. Repeat testing may be done once these conditions have resolved to determine whether the proteinuria is persistent.
If trace amounts of protein are detected, and depending on the person’s signs, symptoms and medical history, a repeat urinalysis and dipstick protein may be performed at a later time to see if there is still protein in the urine or if it has dropped back to undetectable levels.
If a large amount of protein is detected on a urinalysis and/or if the protein persists in repeated tests, a 24-hour urine protein test may be used as a follow-up test. Since the dipstick primarily measures albumin, the 24-hour urine protein test also may be ordered if a healthcare practitioner suspects that proteins other than albumin are being released into the urine.
Protein in the urine may be a sign of kidney disease. Small amounts of albumin may be found in the urine when kidney dysfunction begins to develop. A different test called a urine albumin test detects and measures small amounts of albumin in the urine. The urine albumin test is more sensitive than a dipstick urinalysis and is routinely used to screen people with chronic conditions that put them at risk for kidney disease, such as diabetes and high blood pressure.
Proteinuria may also be associated with many other diseases and conditions. A healthcare practitioner may order other types of follow-up tests to help determine the cause of protein in the urine.
Glucose
Glucose is normally not present in urine. When glucose is present, the condition is called glucosuria. It results from either:
- An excessively high glucose level in the blood, such as may be seen with people who have uncontrolled diabetes
- A reduction in the “renal threshold;” when blood glucose levels reach a certain concentration, the kidneys begin to eliminate glucose into the urine to decrease blood concentrations. Sometimes the threshold concentration is reduced and glucose enters the urine sooner, at a lower blood glucose concentration.
Some other conditions that can cause glucosuria include hormonal disorders, liver disease, medications, and pregnancy. When glucosuria occurs, other tests such as a fasting blood glucose are usually performed to further identify the specific cause.
Ketones
Ketones are not normally found in the urine. They are intermediate products of fat metabolism. They are produced when glucose is not available to the body’s cells as an energy source. They can form when a person does not eat enough carbohydrates (for example, in cases of fasting, starvation, or high-protein diets) or when a person’s body cannot use carbohydrates properly. When carbohydrates are not available, the body metabolizes fat instead to get the energy it needs to keep functioning. Strenuous exercise, exposure to cold, frequent, prolonged vomiting, and several digestive system diseases can also increase fat metabolism, resulting in ketonuria.
In a person who has diabetes, ketones in urine may also be an early indication of insufficient insulin. With insufficient insulin, a diabetic cannot process glucose and instead metabolizes fat. This can cause ketones to build up in the blood, resulting first in ketosis and then progressing to ketoacidosis, a form of metabolic acidosis. Excess ketones and glucose are dumped into the urine by the kidneys in an effort to flush them from the body. This condition, called diabetic ketoacidosis (DKA), is most frequently seen with uncontrolled type 1 diabetes and can be a medical emergency.
Blood (Hemoglobin) and Myoglobin
This test is used to detect hemoglobin in the urine (hemoglobinuria). Hemoglobin is an oxygen-transporting protein found inside red blood cells (RBCs). Its presence in the urine indicates blood in the urine (known as hematuria).
A small number of red blood cells are normally present in urine and usually result in a “negative” chemical test. An increased amount of hemoglobin and/or increased number of red blood cells are detected as a “positive” chemical test result. Results of this test are typically interpreted along with those from the microscopic examination of the urine to determine whether red blood cells are present in the urine. A positive result on this test with no red blood cells present may indicate the presence of hemoglobin in the urine (which can occur when red blood cells have broken apart) or myoglobin from muscle injury.
Blood in the urine is not a normal finding, but it is not uncommon and not necessarily a cause for alarm. Your healthcare practitioner will investigate further to try to determine the source and underlying cause of the blood and may request repeat testing to determine whether the blood is persistent.
See “The Microscopic Examination: Red Blood Cells” below.
Leukocyte esterase
Leukocyte esterase is an enzyme present in most white blood cells. A few white blood cells are normally present in urine and usually give a negative chemical test result. When the number of white blood cells in urine increases significantly, the urine screening test will become positive. Results of the urine screening test will be considered along with a microscopic examination for white blood cells in the urine.
When the urine screening is positive and/or the white blood cell count in urine is high, it may indicate that there is inflammation in the urinary tract or kidneys. The most common cause for white blood cells in urine (leukocyturia) is a bacterial urinary tract infection (UTI), such as a bladder or kidney infection. In addition to white blood cells, bacteria and red blood cells may also be seen in the microscopic examination. If bacteria are present, the chemical test for nitrite may also be positive.
Nitrite
The urine screening test detects nitrite and is based upon the fact that many bacteria can convert nitrate (a normal substance in urine) to nitrite. Normally, the urinary tract and urine are free of bacteria and nitrite. When bacteria enter the urinary tract, they can cause a urinary tract infection. A positive nitrite test result can indicate a urinary tract infection (UTI). However, since not all bacteria are capable of converting nitrate to nitrite, someone can still have a urinary tract infection (UTI) despite a negative nitrite test. The results of this test will be considered along with the leukocyte esterase (above) and a microscopic urine examination.
Ascorbic Acid (Vitamin C)
Occasionally, people taking vitamin C or multivitamins may have large amounts of ascorbic acid in their urine. When this is suspected to be the case, a laboratorian may test the sample for ascorbic acid (vitamin C) because it has been known to interfere with the accuracy of some of the results of the chemical test strip, causing them to be falsely low or falsely negative. Examples of tests that may be affected include the urine dipstick tests for glucose, blood, bilirubin, nitrite, and leukocyte esterase.
Microscopic examination
A microscopic examination may or may not be performed as part of a routine urinalysis. It will typically be done when there are abnormal findings on the physical or chemical examination and the results from all will be taken into account for interpretation.
The microscopic exam is performed on urine sediment – urine that has been centrifuged to concentrate the substances in it at the bottom of a tube. The fluid at the top of the tube is then discarded and the drops of fluid remaining are examined under a microscope. Cells, crystals, and other substances are counted and reported either as the number observed “per low power field” (LPF) or “per high power field” (HPF). In addition, some entities, if present, are estimated as “few,” “moderate,” or “many,” such as epithelial cells, bacteria, and crystals. Cells and other substances that may be seen are listed below.
Red blood cells
Normally, a few red blood cells are present in urine sediment (0-5 red blood cells per high power field, HPF). A positive chemical test for hemoglobin and an increase in the number of red blood cells seen under the microscope indicates that there is blood in the urine. However, this test cannot be used to identify where the blood is coming from. For instance, contamination of urine with blood from hemorrhoids or vaginal bleeding cannot be distinguished from a bleed in the urinary tract. This is why it is important to collect a urine specimen correctly and for women to tell their healthcare provider that they are menstruating when asked to collect a urine specimen.
Blood in the urine is not a normal finding, but it is not uncommon and is not necessarily a cause for alarm. Hematuria is a sign or an indicator that prompts a healthcare practitioner to investigate further to try to determine the underlying cause of the blood. As part of the investigation, a healthcare practitioner will evaluate an individual’s medical history, physical examination, and accompanying signs and symptoms. Additional urine and blood tests may be done to help determine the source.
Some of the underlying causes of hematuria are benign, temporary states that do no lasting harm and resolve with little or no specific treatment. If there is blood in the urine along with white blood cells and bacteria, it may be caused by a urinary tract infection that can be easily treated with antibiotics. Some causes of hematuria, however, may be critical conditions or represent a chronic condition that requires treatment and monitoring.
White blood cells
The number of white blood cells in urine sediment is normally low (0-5 white blood cells per high power field, HPF). White blood cells can be a contaminant, such as those from vaginal secretions.
An increased number of white blood cells seen in the urine under a microscope and/or positive test for leukocyte esterase may indicate an infection or inflammation somewhere in the urinary tract. If also seen with bacteria (see below), they indicate a likely urinary tract infection.
Epithelial cells
Epithelial cells are usually reported as “few,” “moderate,” or “many” present per low power field (LPF). Normally, in men and women, a few epithelial cells can be found in the urine sediment. In urinary tract conditions such as infections, inflammation, and malignancies, an increased number of epithelial cells are present. Determining the kinds of cells present may sometimes help to identify certain conditions. For example, epithelial cells containing large amounts of broken-down hemoglobin (called hemosiderin) may indicate that there were red blood cells or hemoglobin in the urine recently, even if there are none now.
Bacteria, yeast and parasites
In healthy people, the urinary tract is sterile and, if the urine sample is collected as a “clean-catch” sample, there will be no microbes seen in the urine sediment under the microscope. Special care must be taken during specimen collection, particularly in women, to prevent bacteria that normally live on the skin or in vaginal secretions from contaminating the urine sample.
If microbes are seen, they are usually reported as “few,” “moderate,” or “many” present per high power field (HPF).
- Bacteria from the surrounding skin can enter the urinary tract at the urethra and move up to the bladder, causing a urinary tract infection (UTI). If the infection is not treated, it can eventually move to the kidneys and cause kidney infection (pyelonephritis). If a person has an uncomplicated lower urinary tract infection, then the person may be treated without need for a urine culture. However, if the person has had recurrent urinary tract infections, suspected complicated infection, or is hospitalized, a urine culture and susceptibility testing may be performed to help guide treatment.
- In women (and rarely in men), yeast can also be present in urine. They are most often present in women who have a vaginal yeast infection because the urine has been contaminated with vaginal secretions during collection. If yeast are observed in urine, then the person may be treated for a yeast infection.
- Trichomonas vaginalis is a parasite that may be found in the urine of women, or rarely, men. As with yeast, Trichomonas vaginalis infects the vaginal canal and their presence in urine is due to contamination during sample collection. If these are found during a urinalysis, then Trichomonas testing may be performed to look for a vaginal infection.
Casts
Casts are cylindrical particles sometimes found in urine that are formed from coagulated protein released by kidney cells. They are formed in the long, thin, hollow tubes of the kidneys known as tubules and usually take the shape of the tubule (hence the name). Under the microscope, they often look like the shape of a “hot dog” and in healthy people they appear nearly clear. This type of cast is called a “hyaline” cast. Normally, healthy people may have a few (0–5) hyaline casts per low power field (LPF). After strenuous exercise, more hyaline casts may be detected.
Other types of casts are associated with different kidney diseases, and the type of casts found in the urine may give clues as to which disorder is affecting the kidney. Cellular casts, such as red blood cell and white blood cell casts, indicate a kidney disorder. Some other examples of types of casts include granular casts, fatty casts, and waxy casts. When a disease process is present in the kidney, cells or other substances can become trapped in the protein as the cast is formed. When this happens, the cast is identified by the substances inside it, for example, as a red blood cell cast or white blood cell cast.
Crystals
Urine contains many dissolved substances (solutes) – waste chemicals that the body needs to eliminate. These solutes can form crystals, solid forms of a particular substance, in the urine if:
- The urine pH is increasingly acidic or basic;
- The concentration of dissolved substances is increased; and
- The urine temperature promotes their formation.
Crystals are identified by their shape, color, and by the urine pH. They may be small, sand-like particles with no specific shape (amorphous) or have specific shapes, such as needle-like. Crystals are considered “normal” if they are from solutes that are typically found in the urine; these usually form as urine cools after collection and were not present in the body. Some examples of crystals that can be found in the urine of healthy individuals include:
- Amorphous urates
- Crystalline uric acid
- Calcium oxalates
- Amorphous phosphates
If the crystals are from substances that are not normally in the urine, they are considered “abnormal.” Abnormal crystals may indicate an abnormal metabolic process. Some of these include:
- Calcium carbonate
- Cystine
- Tyrosine
- Leucine
Normal or abnormal crystals can form within the kidneys as urine is being made and may group together to form kidney “stones” or calculi. These stones can become lodged in the kidney itself or in the ureters, tubes that pass the urine from kidney to the bladder, causing extreme pain.
Medications, drugs, and x-ray dye can also crystallize in urine. Therefore, the laboratorian must be familiar with and trained in the identification of urine crystals.





{kind=link}