What is otosclerosis
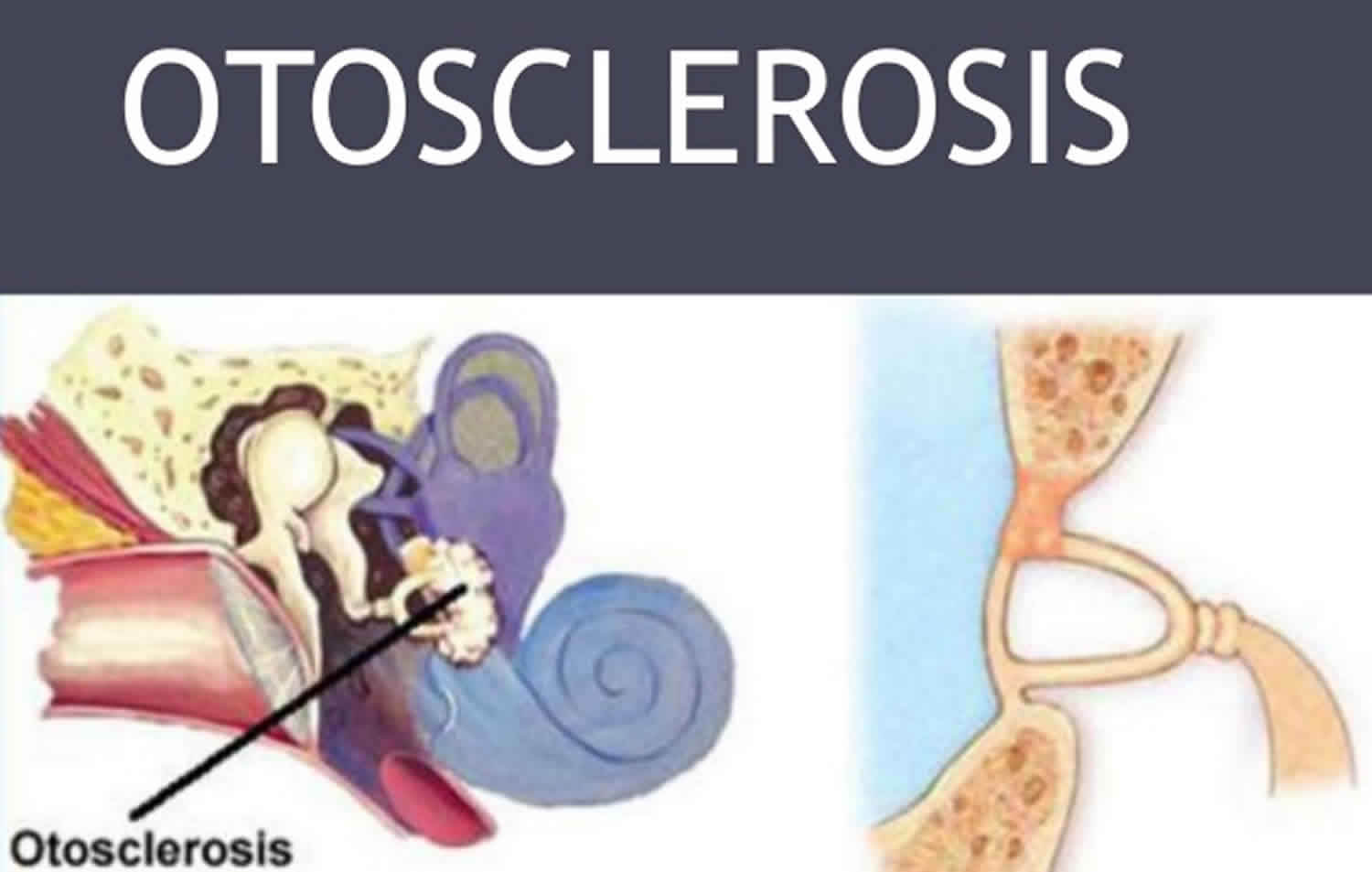
Otosclerosis is an abnormal bone growth in the middle ear that causes progressive conductive hearing loss. Otosclerosis usually affects the last bone in the middle ear called the stapes (specifically at the footplate of the stapes see Figure 3 below) located at the entrance to the cochlea – the organ that senses sound. With otosclerosis, the stapes can ‘stick’ to the cochlea’s entrance and interfere with the mechanical transfer of sound to the inner ear. Fixation causes stiffness enhancement of the ossicular chain. If the abnormal bone growth extends into the inner ear, it can also cause sensorineural hearing loss and affect your balance.
Otosclerosis is the most common cause of middle ear hearing loss in young adults. Otosclerosis typically begins in early to mid-adulthood between 15 and 30 years. Otosclerosis is more common in women than in men. Otosclerosis may affect one or both ears.
Pregnancy can cause Otosclerosis to progress more rapidly.
Risks for otosclerosis include pregnancy and a family history of hearing loss. White people are more likely to develop otosclerosis than people of other races.
Appropriate management options for the conductive hearing loss include either hearing amplification or stapes surgery.
A Bone-Conduction Hearing Aid or a Bone Anchored Hearing Device may be used to treat the hearing loss. This will not cure or prevent hearing loss from getting worse, but it may help with symptoms.
Surgery can cure or improve conductive hearing loss. Either all or part of one of the small middle ear bones behind the eardrum (stapes) is removed and replaced with a prosthesis.
- A total replacement is called a stapedectomy.
- Sometimes only part of the stapes is removed and a small hole is made in the bottom of it. This is called a stapedotomy. Sometimes a laser is used to help with the surgery.
Human hearing mechanism
The ear consists of the outer, middle and inner ear. Sound travels through the outer ear and reaches the eardrum, causing it to vibrate. The vibration is then transmitted through three tiny bones in the middle ear called the ossicles. These three ossicles are called malleus, incus and stapes, sometimes known as hammer, anvil and stirrup. The vibration then enters the inner ear which is a snail-shaped bony structure filled with fluid. The nerve cells within the inner ear are stimulated to produce nerve signals. These nerve signals are carried to the brain, where they are interpreted as sound.
There are two auditory systems in human hearing mechanism, the peripheral and the central systems. The ear is part of the peripheral auditory system, is divided into three main parts – the outer ear, the middle ear, and the inner ear (see Figures 1 to 4). The inner ear is filled with fluid. The inner ear also contains the receptors for sound which convert fluid motion into electrical signals known as action potentials that are sent to the brain to enable sound perception. The airborne sound waves must therefore be channelled toward and transferred into the inner ear for hearing to occur. The role of the outer and middle ear is to transmit sound to the inner ear (Figures 1 to 4). They also help compensate for the loss in sound energy that naturally occurs when the sound waves pass from air into water by amplifying the sound energy during the process of sound transmission. In addition to converting sound waves into nerve action potentials, the inner ear is also responsible for the sense of equilibrium, which relates to our general abilities for balance and coordination.
- The outer ear adjusts the sound wave in transferring the acoustic vibrations to the eardrum with changing of the sound pressure depending on the direction of the sound and resonating the sound pressure in the range of frequencies of 2-7 kHz.
- The middle ear couples the sound energy from the low-impedance air to the higher impedance cochlear fluids acting as a transformer. The middle ear transmits acoustic energy from the external auditory meatus to the cochlea. When the sound enters the middle ear cavity, its acoustic energy is converted into the mechanical energy, then into hydraulic energy when entered to cochlear fluids. In response to much higher impedance of the cochlear fluids, the middle ear allows impedance matching by increasing the pressure. This is called the transfer function of the middle ear. This phenomenon is mainly attributed to two principles. One is the ratio of the area of the tympanic membrane and the oval window and the other is the lever action of two middle ear bones, the malleus and the incus. As the middle ear transforms the sound pressure variation of the ear canal into a sound pressure variation in the scala vestibuli, the transfer function can be shown by plotting the ratio of the two pressures at different stimulus frequencies.
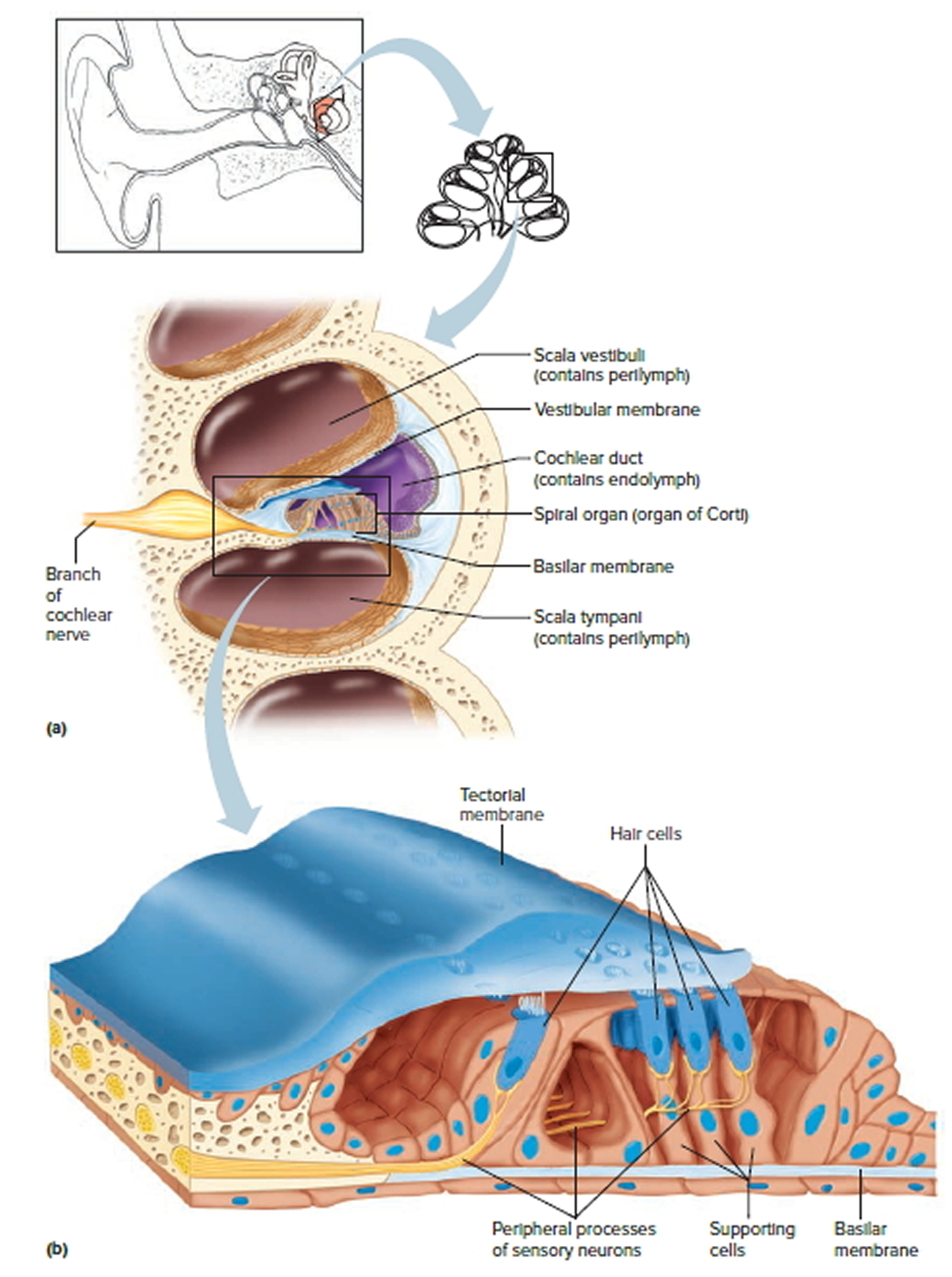
- The inner ear, also known as the cochlea, separates stimulus frequencies into different spatial regions and converts changes in pressure into vibration for the discharge of auditory neurons. Directly responsible for sensory function in the cochlea, the organ of Corti sits on the top of the basilar membrane. A cellular and gelatinous structure, tectorial membrane, covers top of the organ of Corti. These three essential structures for cochlear function, the basilar membrane, the organ of Corti, and the tectorial membrane make up the cochlear partition. Mass and stiffness with the other physical properties of the middle ear and the cochlear partition affect on the peculiar characteristics of transmission of the middle ear and the behavior to different frequencies of stimulation in the cochlear partition.
The effectiveness of transmitting vibration of the sound energy is frequency dependent because every object has a resonant frequency. The resonant frequency is determined by an object’s acoustic impedance limiting a certain frequency transmission. We manipulate this acoustic impedance when we play a musical instrument. Two renowned properties that determine an object’s resonant frequency are mass and stiffness. Mass limits high-frequency transmission, as heavier objects vibrate at lower frequencies while stiffness limits low-frequency transmission, as a less elastic in other words stiff objects vibrate at higher frequencies. For example, a xylophone uses bigger keys for resonance of lower frequencies and in flute, the shorter the column, the resonant frequency becomes higher as changing the length of an air column changes its elasticity. In the peripheral auditory system, the middle ear and the cochlear partition are affected by the mass and stiffness for their unique movement characteristics. When the sound energy transmits in the middle ear, the bones supply mass and volume of the middle ear cavity impinges on stiffness providing band-pass characteristics for the transfer function. Also, depending on its structural nature, the degree of the establishment of gradients for mass and stiffness of the cochlear partition is responsible for the manner of the traveling wave and the distinctive basilar movement.
Converting sound wave vibrations into inner ear fluid movement
As the eardrum vibrates in response to air waves, the chain of inner ear bones are set into motion at the same frequency (see Figure 3). The frequency of movement is transmitted across from the eardrum to the oval window (another structure in the ear), resulting in a pressure being exerted on the oval window with each vibration. This produces wavelike movements of the inner ear fluid at the same frequency as the original sound wave. However, in order to set the fluid into motion, greater pressure is required, so that the pressure must be amplified. This amplification of the pressure of the airborne sound wave to set up fluid vibrations in the cochlea is related to two mechanisms. Firstly, the surface area of the tympanic membrane is much large than that of the oval window. In addition, the lever action of the ossicles greatly increases the force exerted on the oval window. The extra pressure generated through these mechanisms is sufficient to set the cochlea fluid in motion.
Physiology of the middle ear
Concentration of energy
The function of the auditory ossicles in the middle ear is to concentrate the energy of the vibrating eardrum so as to create a greater force per unit area at the oval window, as previously described.
Protection of inner ear
In addition to this, the ossicles and their adjacent muscles also serve a protective function. In response to a loud noise, the tensor tympani pulls the eardrum inward and tenses it. At the same time, the stapedius reduces movement of the stapes. These actions of the muscles are known collectively as the tympanic reflex. This reflex muffles the transfer of vibrations from the eardrum to the oval window. It is thought that the tympanic reflex is an evolutionary adaptation for protection against loud but slowly building noises such as thunder. However, because it has a time delay of about 40 ms, it is not quick enough to protect the inner ear from sudden loud noises such as gunshots. It also does not adequately protect the ears from sustained loud noises such as factory noises or loud music. These noises can irreversibly damage the stereocilia of the hair cells in the inner ear, leading to hearing loss.
Coordinating speech with hearing
The muscles of the middle ear also assist in coordinating speech with hearing, so that the sound of our own speech is not so loud as to damage our inner ear and drown out soft or high-pitched sounds from other sources. Just as we are about to speak, the brain signals the middle ear muscles to contract, dampening the sense of hearing in coordination with the sound of our own voice. This makes it possible to hear other people while we are speaking ourselves.
Figure 1. Ear structure
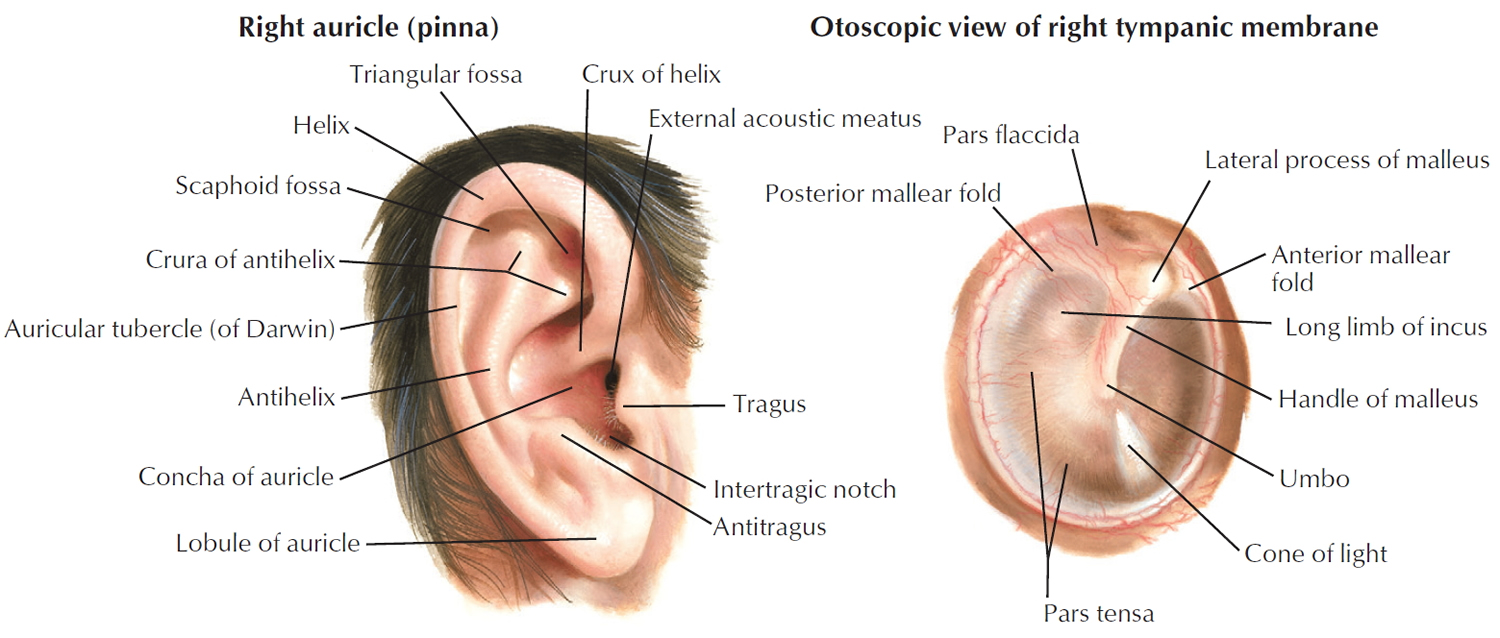
Figure 2. Ear anatomy

Figure 3. Middle ear and auditory ossicles
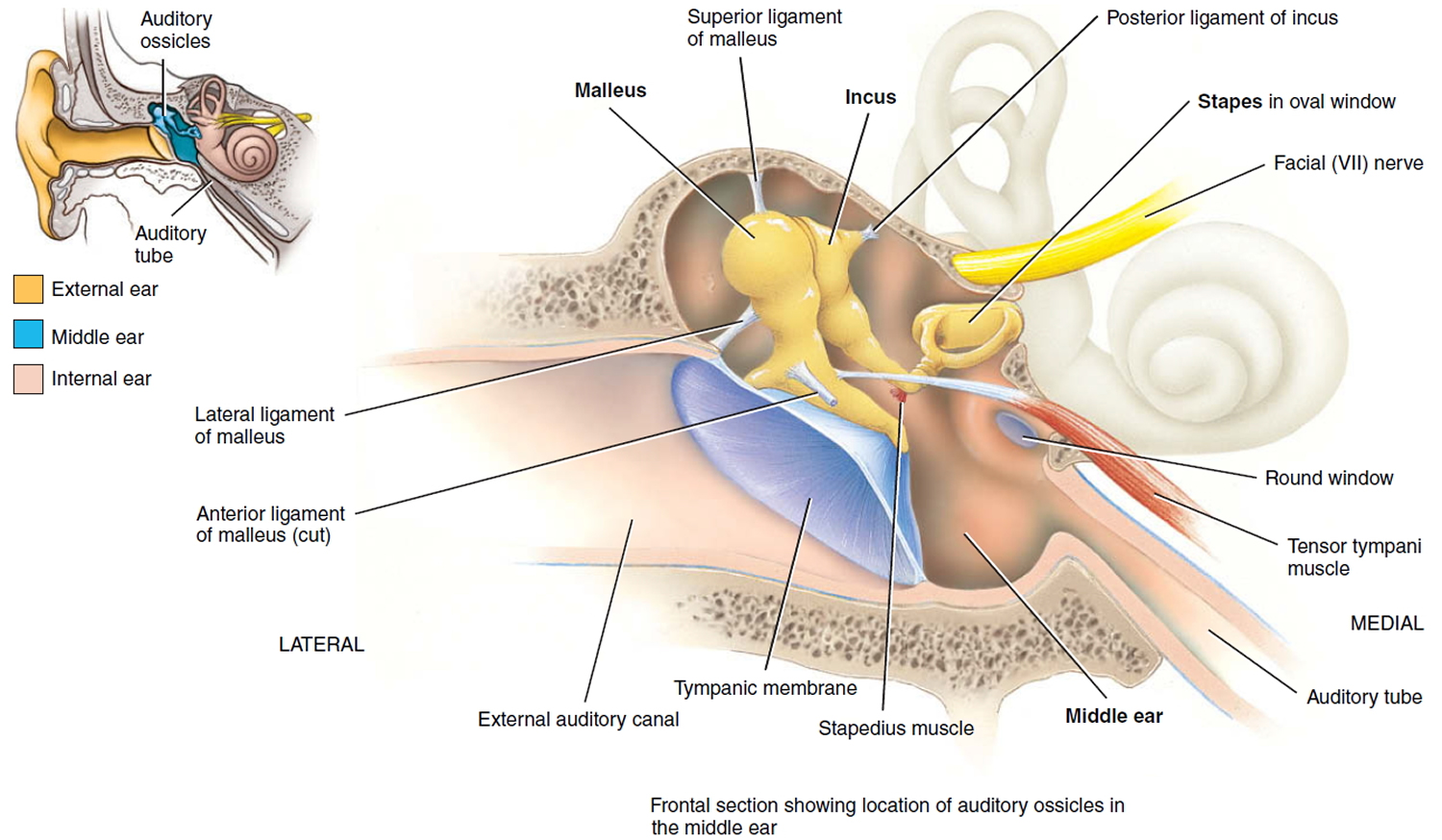
Figure 4. The Cochlea (cross section view)
Otosclerosis causes
The exact cause of otosclerosis is unknown. Otosclerosis may be passed down through families and can be hereditary. People who have a family history of otosclerosis are more likely to develop the disorder. Otosclerosis affects the ears only and not other parts of your body. Both ears are usually involved in some extent. However, in some individuals, only one ear is affected. Otosclerosis usually begins in the teens or early twenties. Some research suggests a relationship between otosclerosis and the hormonal changes associated with pregnancy.
People who have otosclerosis have an abnormal extension of sponge-like bone growing in the middle ear cavity. This growth prevents the ear bones from vibrating in response to sound waves. These vibrations are needed in order for you to hear.
Otosclerosis symptoms
If left untreated, otosclerosis can cause the slow onset of a conductive hearing loss, which can become more severe over time. Tinnitus (ringing noise in the ear) and vertigo (dizziness) can also be associated with otosclerosis. The intensity of the tinnitus is not necessarily related to the degree or type of hearing loss.
Otosclerosis symptoms include:
- Hearing loss (slow at first, but worsens over time)
- Ringing in the ears (tinnitus)
- Vertigo or dizziness
Otosclerosis possible complications
Otosclerosis complications may include:
- Complete deafness
- Funny taste in the mouth or loss of taste to part of the tongue, temporary or permanent
- Infection, dizziness, pain, or a blood clot in the ear after surgery
- Nerve damage
Otosclerosis diagnosis
An examination by an specialist ENT surgeon is needed to rule out other diseases or health problems that may cause these same symptoms. A hearing test (audiometry/audiology) may help determine the severity of hearing loss. Your otolaryngologist may order a CT scan of the ear called a temporal-bone CT to assess the extent of otosclerosis and may be used to look for other causes of hearing loss.
Otosclerosis audiogram
The audiogram with worse air-conduction thresholds at low frequencies, below 1-2 kHz, is typical for otosclerosis 1. Sometimes, in an audiogram with a drop in bone-conduction thresholds at 2 kHz, a “notch” is noted describing a decrease in cochlear sensitivity. This effect, known as the “Carhart’s notch,” actually represents the loss of inertial bone-conduction component as a result of fixation 2. Although some researchers controversially argued whether there is a recovery in bone-conduction thresholds after surgery, the recovery is rather considered the effect of stiffness when the stapes footplate is fixed in position 3.
Figure 5. Otosclerosis audiogram
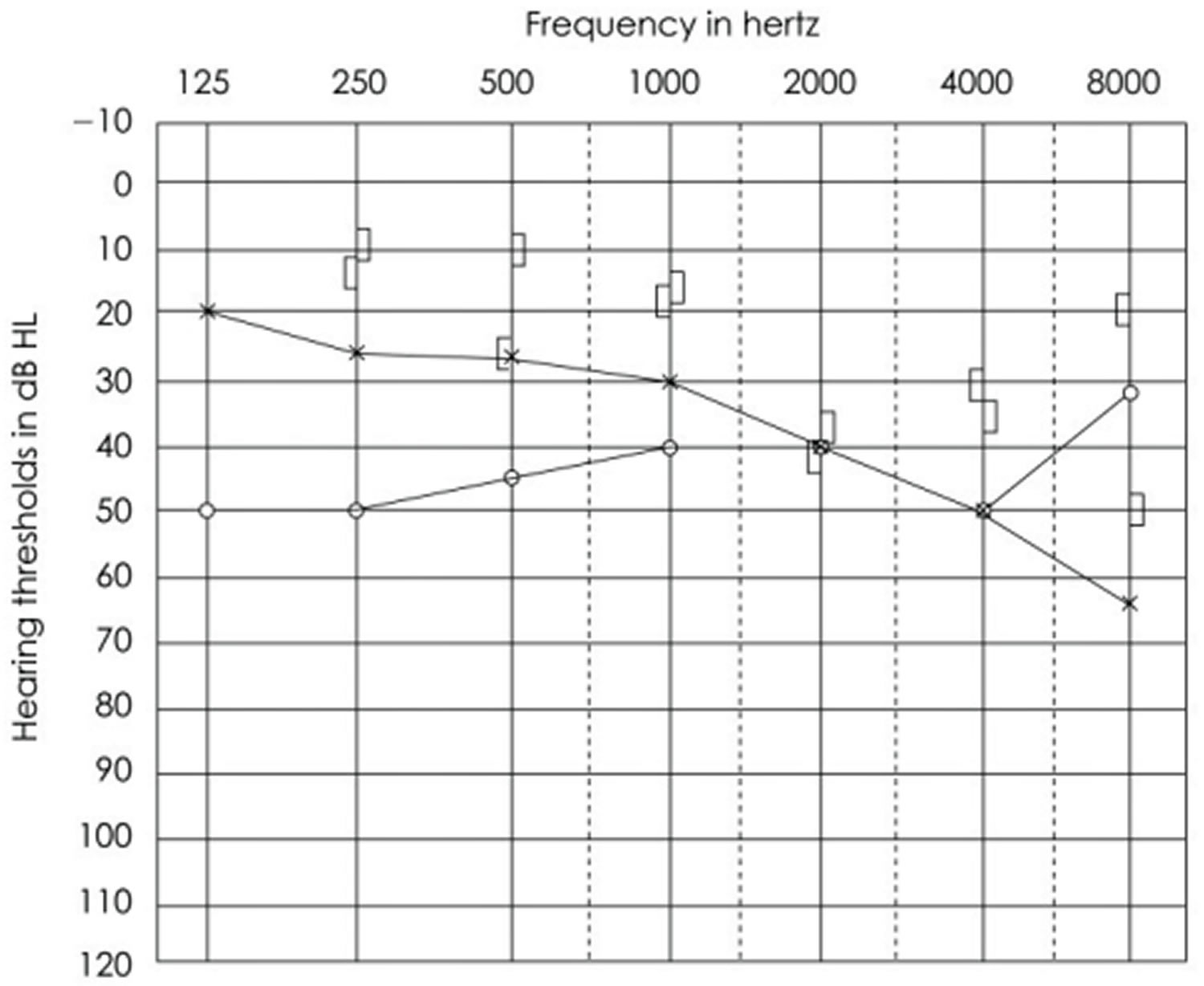
Footnote: An example of audiogram in a patient with otosclerosis on the right ear showing Carhart’s notch.
[Source 4 ]Otosclerosis treatment
Otosclerosis may slowly get worse. The condition may not need to be treated until you have more serious hearing problems.
Using some medicines such as sodium fluoride, calcium, or vitamin D may help to slow the hearing loss. However, the benefits of these treatments have not yet been proven.
The mechanisms postulated regarding fluoride’s activity included antienzymatic activity against proteolytic enzymes 5, reduction of bone resorption 6, changing otospongiotic active lesions to more dense inactive lesions 7 and an increase of new bone formation in the healing process of bone structures.
The adverse reactions reported during fluoride treatment included synovitis, plantar faciitis, gastrointestinal side effects such as recurrent vomiting, peptic ulcer, anemia, and increased skeletal fragility 8.
The sodium fluoride dosage can be adjusted starting with 60 mg and continuing with the maintenance dosage of 20–25 mg if clinical proof of effectiveness of the treatment is seen 9. Derks et al. 10 found out that fluoride treatment is more effective for the higher frequencies in cases with cochlear otosclerosis and an initial sensorineural hearing loss of less than 50dB.
Biphosphonates also have a potential use in the treatment of cochlear otosclerosis by inhibiting the activation of osteoclasts 11. Blookler and Tanyeri 12 reported 70% improvement in their hearing, 54% in dizziness, and 52% in tinnitus in patients with otosclerosis by assessing the efficacy of etidronate, a biphosphonate. Even though the adverse effects are rare, those effects are nausea, ulcers of upper gastrointestinal tract, and similar findings of osteomalacia due to impaired mineralization. In addition, acute renal failure was also reported with IV infusion of etidronate in three patients with malignancies 13.
A Bone-Conduction Hearing Aid or a Bone Anchored Hearing Device may be used to treat the hearing loss. This will not cure or prevent hearing loss from getting worse, but it may help with symptoms.
Otosclerosis surgery
Having ear surgery is another option to remove the hearing loss symptoms associated with the condition. A common ear surgery procedure for otosclerosis is a stapedectomy, which involves removing one of the middle ear bones called the stapes and replacing it with a prosthesis.
The other surgical option is a stapedotomy where only a segment of the stapes is removed and a small hole drilled at the bottom and putting a piston-like prosthesis in place.
You will usually go home the day after the operation or sometimes the same day. A slight amount of dizziness is normal after the operation. The stitches will be removed one to two weeks after the operation. There may be a small amount of discharge from the ear canal. This usually comes from the ear dressings. The packing in the ear canal will be removed after two or three weeks.
You should keep the ear dry for the first few weeks. Plug the ear with a cotton wool ball coated with Vaseline when you are having a shower or washing your hair. Avoid straining for the first few weeks after surgery, that is, no heavy lifting. Only blow the nose gently. Avoid air travel until cleared by your surgeon. Hearing may not return to normal for up to three months. You should consult the surgeon if there is a sudden onset of deafness, dizziness or severe pain after you are discharged from the hospital. You are advised to avoid diving or flying when you have a cold if possible.
You may need to take two to three weeks off work.
Otosclerosis surgery possible complications
There are some risks that you must consider before giving consent to this treatment. These potential complications are rare. You should consult your surgeon about his complication rate.
Loss of hearing
In a small number of patients the hearing may be further impaired due to damage to the inner ear. It can even result in a severe loss of hearing in the operated ear. This may be to the extent that one cannot obtain benefit from a hearing aid in that ear. For experienced surgeons, this complication happens in around one in 100 patients. Therefore the poorer hearing ear is normally selected for surgery first.
Dizziness
Dizziness is common for a few hours following stapedotomy and may result in nausea and vomiting. Some unsteadiness can occur during the first few days following surgery; dizziness on quick head movement may persist for several weeks. On rare occasions, dizziness is prolonged.
Taste disturbance
The taste nerve runs close to the eardrum and may occasionally be damaged. This can cause an abnormal taste on one side of the tongue. This is usually temporary but it can be permanent in one in ten patients.
Tinnitus
Sometimes the patient may notice noise in the ear, in particular if the hearing loss worsens. The uncommon risk of total loss of hearing, disturbance of balance or taste could have a serious implication to certain employments. You should discuss with your specialist about these concerns. Some specialists also advise against scuba diving, sky diving or use of firearm following a stapedotomy operation.
Otosclerosis prognosis
Otosclerosis gets worse without treatment. Surgery can restore some or all of your hearing loss. The chances of obtaining a good result from this operation by experienced surgeons are over 80 percent. This means that eight out of ten patients will get an improvement of hearing up to the level at which their inner ear is capable of hearing. You should enquire from your surgeon his/her personal success rate of otosclerosis surgery. Many surgeons keep a database of their results.
Pain and dizziness from the surgery go away within a few weeks for most people.
To reduce the risk of complications after surgery:
- DO NOT blow your nose for 2 to 3 weeks after surgery.
- Avoid people with respiratory or other infections.
- Avoid bending, lifting, or straining, which may cause dizziness.
- Avoid loud noises or sudden pressure changes, such as scuba diving, flying, or driving in the mountains until you have healed.
If surgery does not work, you may have total hearing loss. Treatment for total hearing loss involves developing skills to cope with deafness, and using hearing aids to transmit sounds from the non-hearing ear to the good ear.
References- Harrell RW. Pure tone evaluation. In: Katz J, Medwetsky L, Burkard RF, Hood LJ, editors. Handbook of Clinical Audiology. 7th ed. Baltimore, USA: Lippincott Williams & Wilkins; 2014. pp. 71–88.
- Carhart R. Atypical audiometric configurations associated with otosclerosis. Trans Am Otol Soc. 1962;50:153–171.
- Kashio A, Ito K, Kakigi A, Karino S, Iwasaki S, Sakamoto T, et al. Carhart notch 2-kHz bone conduction threshold dip: a nondefinitive predictor of stapes fixation in conductive hearing loss with normal tympanic membrane. Arch Otolaryngol Head Neck Surg. 2011;137:236–240.
- Kim J, Koo M. Mass and Stiffness Impact on the Middle Ear and the Cochlear Partition. J Audiol Otol. 2015;19(1):1-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4491943/
- Parahy C, Linthicum FH., Jr Otosclerosis and otospongiosis: clinical and histological comparisons. Laryngoscope. 1984;94:508–512.
- Causse JR, Causse JB, Uriel J, et al. Sodium fluoride therapy. Am J Otol. 1993;14:482–490.
- Bretlau P, Causse J, Causse JB, et al. Otospongiosis and sodium fluoride. A blind experimental and clinical evaluation of the effect of sodium fluoride treatment in patients with otospongiosis. Ann Otol Rhinol Laryngol. 1985;94:103–107.
- Riggs BL, Hodgson SF, O’Fallon WM, et al. Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Engl J Med. 1990;322:802–809.
- Forquer BD, Linthicum FH, Bennett C. Sodium fluoride: effectiveness of treatment for cochlear otosclerosis. Am J Otol. 1986;7:121–125.
- Derks W, De Groot JA, Raymakers JA, Veldman JE. Fluoride therapy for cochlear otosclerosis? an audiometric and computerized tomography evaluation. Acta Otolaryngol. 2001;121:174–177.
- Brookler K. Medical treatment of otosclerosis: rationale for use of bisphosphonates. Int Tinnitus J. 2008;14:92–96.
- Brookler KH, Tanyeri H. Etidronate for the the neurotologic symptoms of otosclerosis: preliminary study. Ear Nose Throat J. 1997;76:371–376. 379–381.
- Bounameaux HM, Schifferli J, Montani JP, et al. Renal failure associated with intravenous diphosphonates. Lancet. 1983;1:471.





{kind=link}