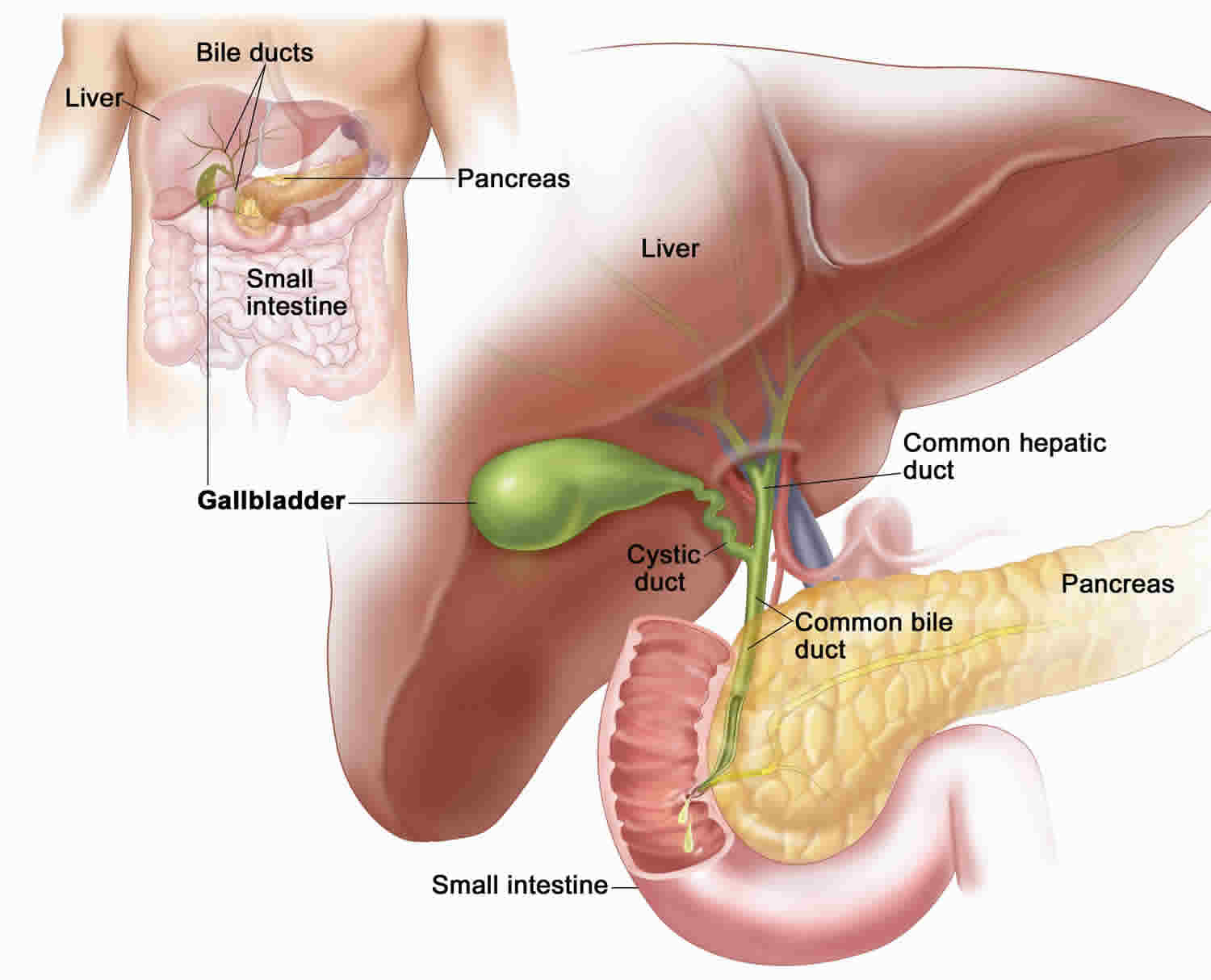
What is a porcelain gallbladder
Porcelain gallbladder also also known as calcified gallbladder or gallbladder calcification, refers to extensive calcium encrustation of the gallbladder wall 1. The porcelain gallbladder term has been used to emphasize the blue discoloration and brittle consistency of the gallbladder wall at surgery, but is often an incidental finding on multiple different imaging modalities. Porcelain gallbladder is a rare finding in 0.05–0.08% of cholecystectomy specimens 2. Porcelain gallbladder is more common in women, between 50 and 70 years, associated with gallstones in 90% of cases and found in <1% of cholecystectomy specimens 3. Types of gallbladder calcification include selective mucosal calcification and diffuse intramural calcification, the latter having a greater affiliation with porcelain gallbladder 4.
Porcelain gallbladder may be associated with gallbladder cancer in over 60% of cases 5 and many asymptomatic patients with confirmed porcelain gallbladder will have a laparoscopic cholecystectomy to treat current or prevent future malignancy 4. However, modern techniques for imaging have led to earlier and more frequent detection of porcelain gallbladder 6, resulting in a much reduced rate of gallbladder cancer among patients with porcelain gallbladder and leading to the suggestion that cholecystectomy is not indicated for asymptomatic porcelain gallbladder 7.
Figure 1. Porcelain gallbladder ultrasound
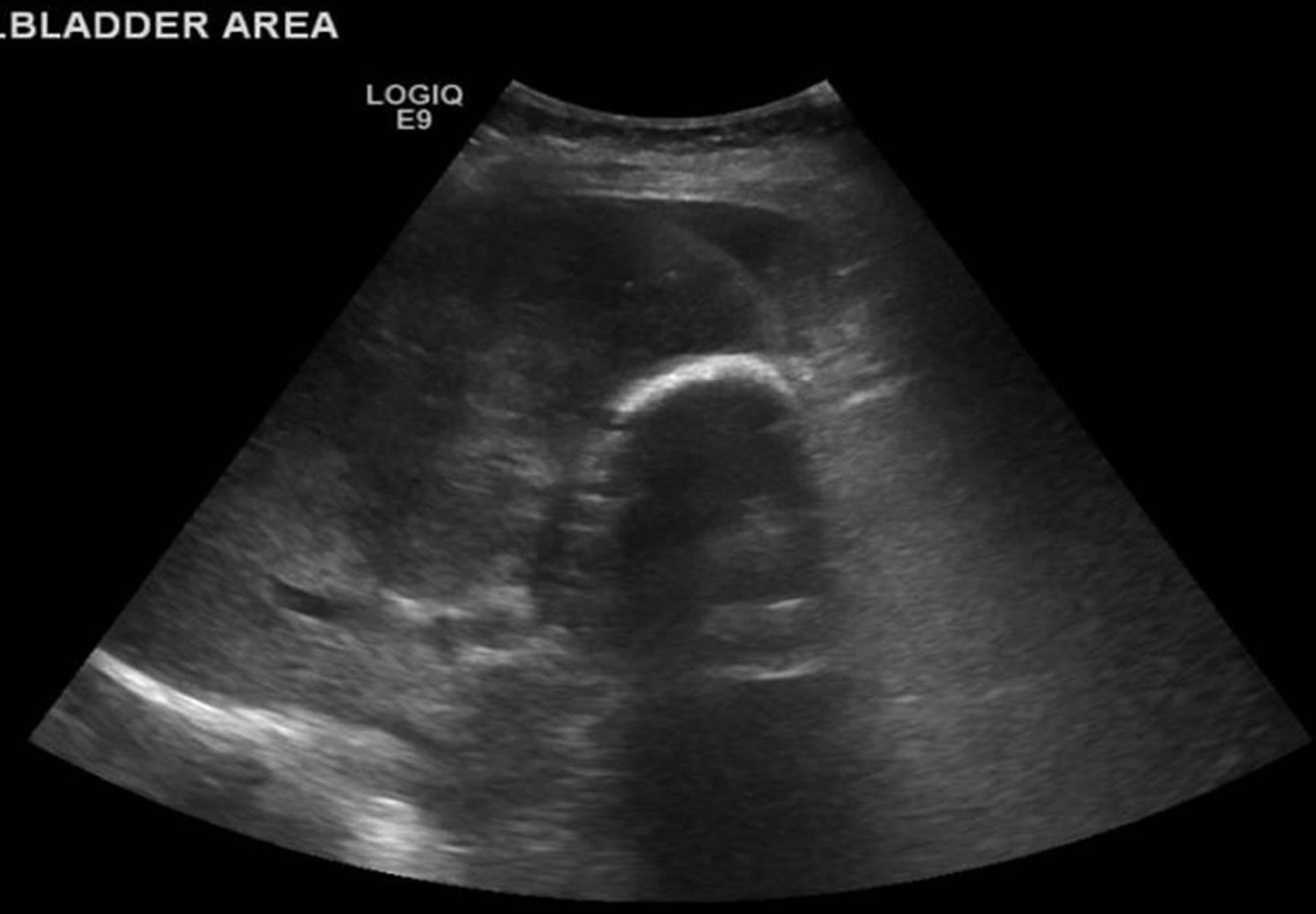
Footnote: Ultrasound showing porcelain gallbladder with a posterior acoustic shadow.
[Source 1 ]Porcelain gallbladder cancer risk
There is no definitive consensus on the incidence rate of gallbladder cancer from porcelain gallbladder but is estimated to range from 12.5% to 61% 8 other studies suggested a lower incidence of 0–5% however in any case, it still represents a statistically significant risk factor of developing gallbladder cancer 4. Nonetheless, the causal relationship between porcelain gallbladder and gallbladder cancer has not been established. Studies have shown that porcelain gallbladder has a weaker association with gallbladder carcinoma than once thought 9. The development of gallbladder cancer in addition to porcelain gallbladder is associated with other risk factors, including gallstones of >3.0 cm in size, cholecystoenteric fistulae, an anomalous pancreaticobiliary junction, gallbladder adenomas or polyps, choledochal cysts, occupational exposure to carcinogens and chronic Salmonella typhi infections 8.
A recent systematic review by Schnelldorfer 10 studied the association of porcelain gallbladder with gallbladder cancer; of 111 articles detailing 340 patients with gallbladder wall calcification, the incidence of gallbladder malignancy was 21%. While the author noted that patients with calcified gallbladders were indeed statistically at risk of developing gallbladder malignancy, on careful analysis of the data, the actual risk of malignancy was significantly less. Moreover, Schnelldorfer 10 indicated certain limitations which could have resulted in an overestimation in the reported incidence of gallbladder cancer among patients with porcelain gallbladder, including: (1) publication bias, in that publishers might prefer to publish rare or ‘curious’ cases only; (2) selection bias, whereby researchers selected subjects from a population of gallbladder cancer patients rather than from the general population or because most reported patients were published in case series and thus did not include a systematic selection of patients; and (3) sampling bias, as most studies represented institutional experiences of patients with gallbladder-related symptoms seeking medical advice. These factors are further compounded by the fact that most gallbladder wall calcifications are asymptomatic, and hence undiagnosed, resulting in an underreporting of benign cases 10. In a subgroup analysis of 13 studies without obvious selection bias, the rate of gallbladder malignancy was noted to be only 6% (0–33%) in patients with gallbladder calcification compared to 1% (0–4%) in a matched cohort of patients without gallbladder calcification 10.
Porcelain gallbladder causes
Its exact cause of porcelain gallbladder is poorly understood, however porcelain gallbladder is thought to be as a result of chronic inflammation of the gallbladder wall 11. Errors in calcium metabolism and abnormal calcification are implicated in the formation of porcelain gallbladder such as obstruction of cystic ducts leading to calcium deposits in the mucosa, subsequent degeneration and regeneration process within gallbladder epithelium or offensive chemicals in stagnant bile salts which may lead to mucosal dysplasia and later progress to cancer 1. Carcinomas associated with porcelain gallbladder are diffusely infiltrating adenocarcinomas 12.
Porcelain gallbladder symptoms
Porcelain gallbladder patients are usually asymptomatic and porcelain gallbladder is usually found incidentally on plain abdominal radiographs, ultrasound, or CT images 1. Among 44 patients with porcelain gallbladder, Stephen et al. 8 noted that nonspecific symptoms of a calcified gallbladder included abdominal pain alone (47%), abdominal pain, nausea and vomiting (16%), abdominal pain and fever (9%), abdominal pain and jaundice (5%) and anorexia, nausea and vomiting (5%); however, 18% of patients were asymptomatic.
Porcelain gallbladder diagnosis
The radiological appearance of a porcelain gallbladder varies based on the extent and location of calcification. Ultrasound is useful for identifying abdominal pathologies, however, the diagnosis can be challenging because there are several common differentials such as large opaque gallstones, acute cholecystitis or calcified liver/renal cysts which may closely mimic porcelain gallbladder. In addition, the findings on ultrasound can be non-specific 13.
Although most porcelain gallbladders are incidentally seen on plain abdominal radiographs, the definition and sensitivity provided by CT scanning appears to be far superior to the definition and sensitivity of radiography. CT scan is also superior to radiography for staging gallbladder carcinoma when it is a complication of porcelain gallbladder 14.
Ultrasounds do not depict porcelain gallbladder as well as CT scans do; sonographic findings can mimic those seen with a nonfunctioning gallbladder, large calculus, and emphysematous cholecystitis. Patients with emphysematous cholecystitis usually have diabetes with no point tenderness (ie, diabetic neuropathy). In one third of these patients, the white blood cell count is within the normal range. High-level echoes that outline the gallbladder result from gas within the gallbladder wall. With emphysematous cholecystitis, the male-to-female ratio is 5:1.) 15.
Occasionally, hepatobiliary surgeons may order angiograms when a malignant change has occurred and staging is required.
Radionuclide uptake images obtained with technetium-99m hepatoiminodiacetic acid (HIDA) demonstrate a nonfunctioning gallbladder. Porcelain gallbladder has been detected on bone scans 16. Nuclear medicine findings are nonspecific because HIDA uptake shows nonfunction in acute cholecystitis and chronic cholecystitis. HIDA uptake scanning is not a recommended imaging procedure for the assessment of porcelain gallbladder.
Porcelain gallbladder treatment
Management of porcelain gallbladders has been controversial with no clear guidelines for many decades 1. Although the traditionally perceived strong association with gallbladder cancer, sometimes quoted at over 60%, mandated prophylactic cholecystectomy, this was largely based on papers from before 1962 and newer evidence suggests a much lesser association which may indicate a more selective or an observational approach 17. A review from 2013 found gallbladder cancer in only 6% (0–33%) of porcelain gallbladder compared to 1% (0–4%) in a matched cohort of patients without gallbladder wall calcification 18. It is also noteworthy that the vast majority of gallbladder cancer do not exhibit calcification, a series of 88 gallbladder cancer not finding any such cases 19.
With an overall risk of malignancy of 0.8–6% among patients with porcelain gallbladder, the role of a prophylactic cholecystectomy is debatable 10. Moreover, the risk of major complications following a laparoscopic cholecystectomy favors a nonoperative approach 20. Proponents of a prophylactic cholecystectomy emphasize the benefit of removing the gallbladder and thus eliminating any early undetected malignancies at a potentially curative stage 21. Such an approach could achieve both a better long-term outcome and avoid the potential legal issues associated with delayed management. Therefore, for patients who are relatively young and fit, a prophylactic cholecystectomy is a reasonable option; however, for those whose perceived risk of perioperative morbidity or mortality is greater than the 6% risk of developing malignancy, a nonoperative approach is advisable 10. Nevertheless, it is important to note that patients who are managed conservatively may require close follow-up with frequent radiological imaging to detect malignancy. In addition, the failure to eject bile due to a calcified gallbladder might lead to gallstone formation 10. The role of a hepatobiliary scan in assessing the ejection fraction of the gallbladder in such patients is not clear 22.
During a prophylactic cholecystectomy on patients with porcelain gallbladder, the cholecystectomy specimen should be subjected to frozen section/histopathological examination. If this reveals a malignancy, then a conversion to an extended/radical cholecystectomy should be carried out by wedge resection of liver tissue and the gallbladder bed, followed by a lymphadenectomy 23. In a recent report, Kapoor et al. 23 recommended an anticipatory extended cholecystectomy in patients whose gallbladder wall thickness was >3 mm on radiological imaging and in whom the possibility of malignancy could not be ruled out. This procedure involves the removal of a 2 cm wedge of segments IVb and V of the adjoining liver and a subsequent lymphadenectomy if the frozen section confirms malignancy. Using this approach, the cholecystohepatic plane is not breached and it is possible to perform an en masse removal of the malignant lesion; resection of the adjoining liver en masse prevents the possible microscopic infiltration of gallbladder cancer into the liver 23.
References- Thakrar R, Monib S, Pakdemirli E, Thomson S. Calcified gallbladder cancer: is it preventable?. J Surg Case Rep. 2019;2019(3):rjz069. Published 2019 Mar 22. doi:10.1093/jscr/rjz069 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6439505
- Porcelain gallbladder: ultrasound and CT appearance. Kane RA, Jacobs R, Katz J, Costello P. Radiology. 1984 Jul; 152(1):137-41.
- Porcelain gallbladder. Opatrny L. CMAJ. 2002 Apr 2; 166(7):933.
- Porcelain gallbladder: a benign process or concern for malignancy? Schnelldorfer T. J Gastrointest Surg. 2013 Jun; 17(6):1161-8.
- Porcelain Gallbladder: Decoding the malignant truth. Machado NO. Sultan Qaboos Univ Med J. 2016 Nov; 16(4):e416-e421.
- The role of diffusion-weighted examination in non-polyploid gallbladder malignancies: A preliminary study. Solak A, Solak I, Genç B, Sahin N. Turk J Gastroenterol. 2013; 24(2):148-53.
- Porcelain Gallbladder: No Longer an Indication for Prophylactic Cholecystectomy. Chen GL, Akmal Y, DiFronzo AL, Vuong B, O’Connor V. Am Surg. 2015 Oct; 81(10):936-40.
- Carcinoma in the porcelain gallbladder: a relationship revisited. Stephen AE, Berger DL. Surgery. 2001 Jun; 129(6):699-703.
- Cox M, Patel M, Joneja U, Shaw C, O’Kane P. Focal disruption in the wall of the porcelain gallbladder: a sign of gallbladder carcinoma. Intern Emerg Med. 2016 Dec 8.
- Schnelldorfer T. Porcelain gallbladder: A benign process or concern for malignancy? J Gastrointest Surg. 2013;17:1161–8. doi: 10.1007/s11605-013-2170-0
- Reassessing the need for prophylactic surgery in patients with porcelain gallbladder: case series and systematic review of the literature. Khan ZS, Livingston EH, Huerta S. Arch Surg. 2011 Oct; 146(10):1143-7.
- Porcelain Gallbladder Mimicking Carcinoma Gallbladder-a Case Report and Review of Literature. Shivanna Puttasubbappa P, Pallavi P. Indian J Surg. 2013 Jun; 75(Suppl 1):208-9.
- An often overlooked diagnosis: imaging features of gallbladder cancer. Pilgrim CH, Groeschl RT, Pappas SG, Gamblin TC. J Am Coll Surg. 2013 Feb; 216(2):333-9.
- Ash-Miles J, Roach H, Virjee J, Callaway M. More than just stones: a pictorial review of common and less common gallbladder pathologies. Curr Probl Diagn Radiol. 2008 Sep-Oct. 37(5):189-202.
- Tsai MJ, Chen JD, Tiu CM, Chou YH, Hu SC, Chang CY. Can acute cholecystitis with gallbladder perforation be detected preoperatively by computed tomography in ED? Correlation with clinical data and computed tomography features. Am J Emerg Med. 2009 Jun. 27(5):574-81.
- Scheiner JD, Dupuy DE. Porcelain gallbladder detected on bone scan. Clin Nucl Med. 1998 Dec. 23(12):845-6.
- Porcelain Gallbladder: Is Observation a Safe Option in Select Populations? DesJardins H, Duy L, Scheirey C, Schnelldorfer T. J Am Coll Surg. 2018 Jun; 226(6):1064-1069.
- Schnelldorfer T. Porcelain gallbladder: a benign process or concern for malignancy? J Gastrointest Surg 2013;17:1161–8. 10.1007/s11605-013-2170-0
- Towfigh S, McFadden DW, Cortina GR, Thompson JE Jr., Tompkins RK, Chandler C, et al. Porcelain gallbladder is not associated with gallbladder carcinoma. Am Surg 2001;67:7–10
- Khan ZS, Livingston EH, Huerta S. Reassessing the need for prophylactic surgery in patients with porcelain gallbladder: Case series and systematic review of the literature. Arch Surg. 2011;146:1143–7. doi: 10.1001/archsurg.2011.257
- Cavallaro A, Piccolo G, Panebianco V, Lo Menzo E, Berretta M, Zanghì A, et al. Incidental gallbladder cancer during laparoscopic cholecystectomy: Managing an unexpected finding. World J Gastroenterol. 2012;18:4019–27. doi: 10.3748/wjg.v18.i30.4019
- Kane RA, Jacobs R, Katz J, Costello P. Porcelain gallbladder: Ultrasound and CT appearance. Radiology. 1984;152:137–41. doi: 10.1148/radiology.152.1.6729103
- Kapoor VK, Singh R, Behari A, Sharma S, Kumar A, Prakash A, et al. Anticipatory extended cholecystectomy: The ‘Lucknow’ approach for thick walled gall bladder with low suspicion of cancer. Chin Clin Oncol. 2016;5:8. doi: 10.3978/j.issn.2304-3865.2016.02.07





{kind=link}