
Silicone granuloma
Silicone granuloma also called siliconoma, is a small area of inflammation from silicone. Silicone granuloma is a recognized complication of ruptured silicone breast implants. Silicone granulomas manifest clinically as recurrent cellulitis-like reactions with pain, induration, nodules, ulceration, and local lymphadenopathy (enlarged lymph nodes) 1. Systemic complications have also been reported, including acute pneumonitis, granulomatous hepatitis, organ compression, and sudden death secondary to intravascular embolization 2. In August 1991, the Food and Drug Administration (FDA) prohibited the marketing or sale of injectable liquid silicone for cosmetic purposes 3. Notably, the FDA has never approved the use of injections of liquid silicone for cosmetic treatment in patients. In 1992, the FDA officially banned the use of all silicone injection products in medical procedures 4. However, liquid silicone injection for breast augmentation continues to be performed illegally, making it difficult to estimate the number of females who have received this procedure 5.
Liquid silicone (dimethyl polysiloxane) has been used for soft tissue augmentation for more than 50 years 6. Pure liquid silicone is nontoxic, noncarcinogenic, chemically inert and does not support the growth of microorganisms 7. It is easily injectable, permanent, and inexpensive 2. Liquid silicone has never been approved for use as a soft tissue filler in the United States but is approved by the Food and Drug Administration (FDA) for intraocular injection and is being used off-label as a filler for facial wrinkles and in investigational protocols for human immunodeficiency virus–related lipoatrophy and severe facial deformities 8.
There is enormous controversy regarding the safety of silicone 7. There have been numerous reports of severe complications following liquid silicone injection for soft tissue augmentation. Most of these problems have occurred following the injection of massive volumes of impure, questionable-grade, adulterated silicone (or other viscous fluids purported to be silicone) into the breasts, buttocks, hips, and legs performed by unqualified laypersons in nonmedical facilities. Proponents argue that, when purified sterile silicone is injected by trained medical professionals in minute volumes using the microdroplet serial puncture technique at appropriate intervals, complications are rare. Opponents contend that liquid silicone is a “time bomb” and that disastrous, uncorrectable complications can occur despite good technique, good material, and small amounts injected 9.
Serious reactions to silicone injections have been reported, occurring 3 weeks to 23 years after treatment 10. They are unpredictable and often uncorrectable. They include granulomas, cellulitis, abscesses, draining sinuses, necrosis, scarring, contractures, and deformities 11. While silicone prosthetics are much safer, the pathological response following silicone implant rupture is identical. Silicone granulomas can occur locally, manifest as lymphadenopathy (enlarged lymph nodes) or present at a distant site due to migration of free silicone. If neglected, silicone granulomas can create a firm mass, cause local tissue destruction, ulceration, scarring, and nerve damage 12. Previous literature raised the question of whether silicone granulomas promote cancer or other systemic inflammatory diseases, however, not enough evidence exists to conclusively address the issue 13.
Silicone granuloma was first described in 1964 by Winer et al. 14 after an injection of free silicone used for breast augmentation; silicone granuloma which occurred after ruptured implants were first described in the 1980s. Silicone granulomas due to breast implant rupture can mimic breast cancer both clinically and radiographically 15. As a result of liquid silicone injection to the breast, many females develop inflammatory changes and granulomas, which complicate breast cancer screening 16. Silicone leaking from a ruptured breast implant increases the risk for silicone to transmigrate to different areas. The well-timed removal of an extracapsular silicone is the best treatment because delayed surgery may increase silicone leakage and migration, therefore making complete removal of silicone very difficult or sometimes impossible 17. When silicone leaks out from an implant, the silicone particles spread to local areas, such as to the ipsilateral chest wall, axillary regions and lymph nodes 18. Moreover, silicone can spread to the whole body, sometimes mimicking cancer 14.
While diagnosis of silicone granuloma requires a high index of suspicion, greater awareness of their presentations and complications may prevent unnecessary tests and interventions in appropriate patients. In summary, silicone granuloma can present itself as a soft tissue mass. Cancer is the most important differential diagnosis. Meticulous follow-up is recommended for these patients. Magnetic resonance imaging (MRI) is the preferred study for diagnosis and to rule out cancer although this is frequently very difficult. Positron emission tomography (PET) scans can be falsely positive and core needle biopsies can be inconclusive. The majority of patients should undergo surgery due to symptoms or the inability to rule out cancer 19.
The management of silicone-induced granuloma is often difficult due to migrating silicone and some of the silicone penetrating into the skin reaching the epidermis. In general, the management of granuloma can be categorized into two, i.e., surgical and pharmacological treatments.
Figure 1. Silicone granuloma buttocks
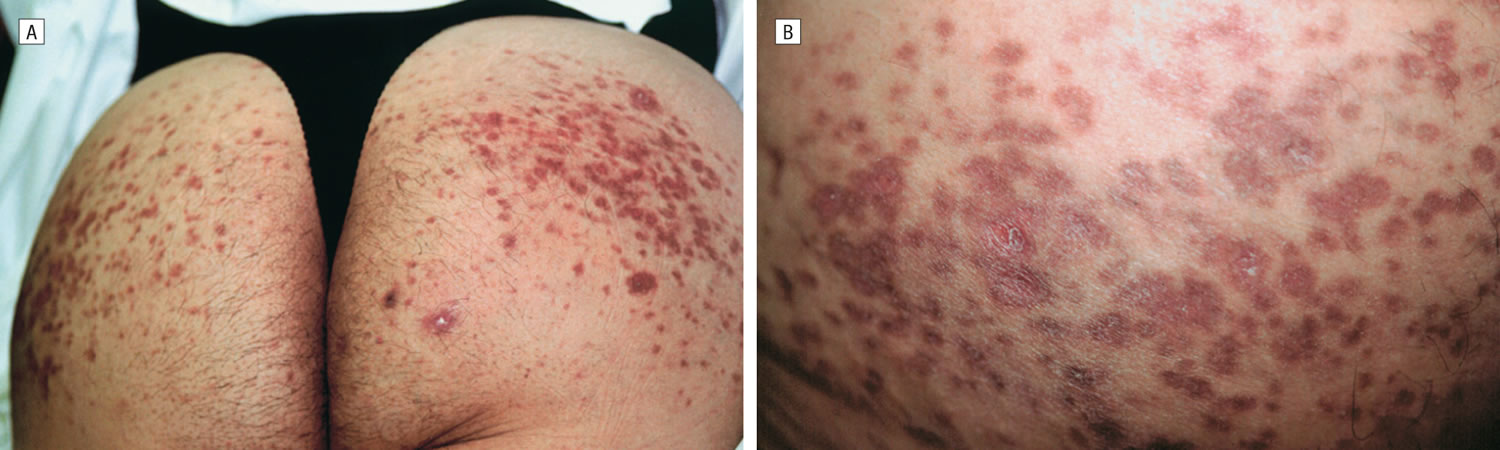
Footnote: A 37-year-old Hispanic woman presented with a 3-month history of painful, exquisitely tender, erythematous nodules and induration of the buttocks. The lesions developed 5 months after she received a series of 3 injections of silicon” into her buttocks at 2-week intervals at a neighborhood spa in upper Manhattan, New York, NY. The patient was severely depressed, complained of pain in her buttocks not relieved by high doses of nonsteroidal anti-inflammatory drugs and hydrocodone, and could not sit, sleep, or work. The patient complained of intolerable, constant pain and was suicidal. She was afebrile and had no lymphadenopathy. (A) Painful, exquisitely tender, subcutaneous nodules with overlying induration of the buttocks 5 months after silicone injections into the site (before treatment). (B) Close-up of indurated plaques. Histopathologic examination of a biopsy specimen of the buttock showed a granulomatous inflammatory infiltrate of lymphocytes, histiocytes, and multinucleated giant cells surrounding lipidlike material, consistent with silicone granuloma. Bacterial, deep fungal, and atypical mycobacterial tissue cultures were negative. Her pain improved tremendously with etanercept; however, the induration and subcutaneous nodules remained unchanged (after 1 month of treatment with etanercept). The patient had resumed her job and was able to sit and sleep comfortably. There was no change in induration or nodularity of her buttocks, but the erythema and tenderness had resolved. She was no longer depressed. At 2-month follow-up, the patient remained in remission.
[Source 6 ]Silicone granuloma breast implants
Breast implants are medical devices that are used to augment breast size or to reconstruct the breast following mastectomy or to correct a congenital abnormality. Breast implants consist of a silicone outer shell and a filler (most commonly silicone gel or saline). Approximately 5 to 10 million women worldwide have breast implants 20. According to the American Society of Plastic Surgeons National Clearinghouse of Plastic Surgery Procedural Statistics, there were 296,203 breast augmentation procedures and 93,083 breast reconstruction procedures performed in the United States in 2010. Approximately half the procedures used saline-filled implants and half used silicone gel-filled implants 20.
Types of breast implants 21
- Saline-Filled breast implants: Saline-filled breast implants contain a silicone outer shell filled with a sterile saltwater (saline) solution. Some are pre-filled and others are filled during the implant operation. Saline-filled implants come in different sizes and have either smooth or textured shells. The FDA approved saline-filled breast implants for breast augmentation in women age 18 or older and for breast reconstruction in women of any age. They are also used in revision surgeries, which correct or improve the result of an original surgery.
- Silicone-Filled breast implants: Silicone gel-filled breast implants have a silicone outer shell that is filled with silicone gel. They come in different sizes and have either smooth or textured shells. Silicone gel-filled breast implants are approved for breast augmentation in women age 22 or older and for breast reconstruction in women of any age. They are also used in revision surgeries, which correct or improve the result of an original surgery.
Silicone granulomas can develop 4 weeks to 16 years following breast implant rupture 19. Silicone granulomas develop as a result of breast implant rupture and present with many of the signs and symptoms of breast cancer. The majority of patients will develop a painless breast or armpit mass. Others will have pain or be diagnosed incidentally during surveillance imaging. The exact prevalence of breast implant rupture is unknown, but is likely underestimated as it can be asymptomatic 12.
The majority of patients should undergo surgery for symptom relief or to rule out cancer 19. Silicone liquid can escape as the prosthetic shell weakens affecting the surrounding breast tissue. It has a tendency to spread and migrate due to its high fat solubility.
Breast implants are not lifetime devices. The longer a woman has implants, the more likely it is that she will need to have surgery to remove or replace them. The most frequent complications and adverse outcomes experienced by breast implant patients include capsular contracture, reoperation, and implant removal (with or without replacement). Other common complications include implant rupture with deflation, wrinkling, asymmetry, scarring, pain, and infection. In addition, women with breast implants may have a very low but increased likelihood of being diagnosed with anaplastic large cell lymphoma 21.
Breast cancer rarely occurs in the form of a foreign body granuloma following liquid silicone injection. This concern has not been substantiated yet. But breast cancer originating from a silicone granuloma has been reported 22. Considering so many women that have breast implants every year; the compiled data show that there is a very small risk of developing non-Hodgkin’s lymphoma and anaplastic large cell lymphoma 23. Moreover, the relationship between breast augmentation and angiosarcoma of the breast remains unclear, but a few cases has been reported in the literature 17. T-cell mediated autoimmune reactions may have some relationship with the silicone implants. But clinical case reports still have been unable to establish a correlation 24.
Silicone granuloma causes
Granuloma is a foreign body reaction against foreign substances that enter the skin. Granuloma occurs due to continuous or chronic inflammation against foreign substances. Silicone is a foreign substance in your body, which will be encapsulated by the body. Datia cells (giant cells) will encapsulate silicone material, and therefore inflammatory mediators cannot perform phagocytosis, which results in continuous inflammation and causes side effect. The encapsulated material has poor vascularization; therefore, it may potentially induce infections.
Silicone granuloma is a foreign body granuloma, which is characterized by the presence of multinuclear Datia cells and macrophages surrounded by lymphocytes and infiltrates of neutrophils. The granulomatous histological lesion caused by silicone varies depending on the type of silicone.
Tissue reactions to silicone gel or liquids are characterized by the formation of silicone granuloma with cystic space containing foreign body 25. The irregular surface of silicone cannot be phagocytosed completely by macrophage. Datia cells are formed due to “frustrated” macrophages. Microspheres in the size of less than 15 microns will be phagocytosed and transferred to the lymph node, while those with big size and nonabsorbable polymer will be encapsulated by fibrotic tissue 26.
Datia cells (giant cells) is essential in tissue response to silicone, in which the Datia cell is phagocytosing the silicone. It appears that although the Datia cell cannot eliminate the silicone, it would produce fragmented silicone into smaller pieces. Within a month, the silicone will be in the size of 20–100 microns 27. However, it still cannot be completely phagocytosed, and ultimately it will be encapsulated by fibrotic tissue.
In general, silicone granuloma can be categorized into three phases according to the natural history of your immune response, which are mild inflammatory phase, i.e., stage 1; inflammation with Datia cells, i.e., stages 2, 3, 4, and 5; and tolerance phase with fibrosis, i.e., stages 6 and 7.
According to Harlim in 2018 28, histopathological features of silicone granuloma can be categorized into seven stages, which are:
- Stage 1, moderate reaction with a few inflammatory cells
- Stage 2, inflammatory cells with one or two Datia cells
- Stage 3, inflammatory cells with more than two Datia cells and <50% fibrotic area
- Stage 4, inflammatory cells with more than two Datia cells and >50% fibrotic area
- Stage 5, inflammatory cells with one Datia cell and >50% fibrotic area
- Stage 6, <50% fibrotic area with no Datia cell
- Stage 7, >50% fibrotic area with no Datia cell
The pathogenesis of silicone granulomas is unknown, although it is believed to involve T-cell activation, possibly triggered by infectious processes, adulterants added to silicone to enhance fibroplasia, or denaturing host proteins adsorbed to silicone. Silicone granulomas are associated with elevated levels of tumor necrosis factor alpha (TNF-α) 29. Tumor necrosis factor alpha (TNF-α) is a proinflammatory cytokine that plays an important role in granuloma formation in many diseases, including sarcoidosis and Crohn disease 30. The TNF inhibitors infliximab and etanercept have been used successfully in patients with sarcoidosis 31. These agents would thus appear to be a promising treatment for silicone granulomas 6.
Silicone granuloma signs and symptoms
Silicone granulomas manifest clinically as recurrent cellulitis-like reactions with pain, induration, nodules, ulceration, and local lymphadenopathy (enlarged lymph nodes) 1. Systemic complications have also been reported, including acute pneumonitis, granulomatous hepatitis, organ compression, and sudden death secondary to intravascular embolization 2.
Silicone granuloma diagnosis
Detection of silicone by imaging methods is challenging for radiologists because presence of silicone breast implant may cause difficulties for breast cancer diagnosis. In addition, breast implant complications can mimic breast cancer.
Breast implant rupture may appear on mammography with mammography demonstrates free or residual silicone in the breast parenchyma. Silicone from incomplete removal surgery of a ruptured implant can be seen as well-circumscribed or ill-defined densities 18. Calcification, architectural distortion, lipid-cyst formation such as fat necrosis, and the thickening and calcification of the skin can be seen as well 32. If mammography is suspected or the result is inconclusive, further evaluation may be needed.
Dynamic contrast-enhanced magnetic resonance imaging (MRI) is the optimal modality to assess for rupture and silicone granuloma formation. An MRI should be done for every patient with breast implants who presents with a breast or armpit mass 33. MRI findings of free silicone include separated foci of low signal intensity on fat-suppressed T1-weighted images and high signal intensity on the water-suppressed T2-weighted images. Typical MRI findings for silicone granulomas include evidence of implant collapse with free silicone particles outside the prosthetic shell and in the tissue surrounding the fibrous shell that forms around the implant. These findings in the context of rupture can reliably diagnose silicone granuloma and exclude breast cancer 34. Contrast enhancement of silicone granulomas on MRI is atypical but occurred in a patient reported by Grubstein et al. 33.
The classic appearance of silicone on sonography is a high echogenic pattern which shows posterior echoes with a well-defined anterior margin and a loss of detail posterior margin. This pattern has been described as “echo-dense noise” or “snowstorm” 35, however, findings may be nonspecific.
The use of positron emission tomography (PET) computed tomography (CT) for oncological surveillance in patients with siliconomas may yield false-positive results; the inflammatory cells of silicone granulomas have increased fluorodeoxyglucose (FDG) uptake from avid glycolysis 36.
Pathological tissue specimens remain the gold standard for diagnosis of silicone granuloma. Biopsy was the final diagnostic step for many patients in our literature review. However, sampling error is always a concern. Multiple biopsies were not sufficient to rule out cancer in our patient given her imaging results. A personal history of breast cancer may also warrant further workup for patients with a negative biopsy 37.
Silicone granuloma treatment
There are no established guidelines for management of silicone granuloma, though excluding cancer is paramount. Treatment of silicone granulomas is difficult and often unsuccessful. Modalities have included intralesional and systemic corticosteroids 11, minocycline 38, imiquimod cream 2, liposuction, lasers, and local resection 1. Surgical removal is the only definitive method of relieving symptoms and avoiding future complications 19. Moreover, surgical excision is often difficult because of migration of silicone to distant sites, resulting in incomplete removal or requiring wide excision 2. An TNF inhibitor etanercept could be of benefit for silicone granulomas, however, further data and experience are needed, and the long-term safety of etanercept must be monitored 6.
References- Hage JJ, Kanhai RC, Oen AL, van Diest PJ, Karim RB. The devastating outcome of massive subcutaneous injection of highly viscous fluids in male-to-female transsexuals. Plast Reconstr Surg. 2001 Mar;107(3):734-41. doi: 10.1097/00006534-200103000-00013
- Baumann LS, Halem ML. Lip silicone granulomatous foreign body reaction treated with aldara (imiquimod 5%). Dermatol Surg. 2003 Apr;29(4):429-32. doi: 10.1046/j.1524-4725.2003.29102.x
- Food and Drug Administration. Current and useful information on collagen and liquid silicone injections. FDA Backgrounder. BG91-20th ed. 1991.
- Peters W, Fomarsier V. Complication from injectable material used for breast augmentation. The Canadian Journal of Plastic Surgery. 2009;17(3):89-96.
- Cheung YC, Lee KF, Ng SH, Chan SC, Wong AM. Sonographic feature s with histologic correlation in two cases of palpable breast cancer after breast augmentation by liquid silicone injection. J Clin Ultrasound. 2002;30:548–51.
- Pasternack FR, Fox LP, Engler DE. Silicone Granulomas Treated With Etanercept. Arch Dermatol. 2005;141(1):13–15. doi:10.1001/archderm.141.1.13
- Duffy DM. Silicone: a critical review. Adv Dermatol. 1990;5:93-107; discussion 108-9.
- Benedetto AV, Lewis AT. Injecting 1000 centistoke liquid silicone with ease and precision. Dermatol Surg. 2003 Mar;29(3):211-4. doi: 10.1046/j.1524-4725.2003.29051.x
- Rapaport M. Silicone injections revisited. Dermatol Surg. 2002 Jul;28(7):594-5. doi: 10.1046/j.1524-4725.2002.22081_2.x
- Rae V, Pardo RJ, Blackwelder PL, Falanga V. Leg ulcers following subcutaneous injection of a liquid silicone preparation. Arch Dermatol. 1989 May;125(5):670-3.
- Bigata XRibera MBielsa IFerrandiz C Adverse granulomatous reaction after cosmetic dermal silicone injection Dermatol Surg 2001;27198- 200.
- Brown SL, Silverman BG, Berg WA. Rupture of silicone-gel breast implants: causes, sequelae, and diagnosis. Lancet. 1997 Nov 22;350(9090):1531-7. doi: 10.1016/S0140-6736(97)03164-4
- Adams ST, Cox J, Rao GS. Axillary silicone lymphadenopathy presenting with a lump and altered sensation in the breast: a case report. J Med Case Rep. 2009 Mar 10;3:6442. doi: 10.1186/1752-1947-3-6442
- Steinbach BG, Hardt NS, Abbitt PL, Lanier L, Caffee HH. Breast implants, common complications, and concurrent breast disease. Radiographics. 1993;13:95–118. https://doi.org/10.1148
- Carson B, Cox S, Ismael H. Giant siliconoma mimicking locally advanced breast cancer: a case report and review of literature. Int J Surg Case Rep. 2018;48:54–60.
- Peters W, Fornasier V. Complications from injectable materials used for breast augmentation. Can J Plast Surg. 2009;17(3):89–96.
- İkizceli T, Gülşen G, Akın İ. Silicone Granuloma Associated with Pectoral Muscle Involvement after Ruptured Breast Implant: a Novel case report. Eur J Breast Health. 2018;14(1):54-57. Published 2018 Jan 1. doi:10.5152/ejbh.2017.3499 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5758066
- Vanwambeke K, Wittevronghel I, Dekeyzer S, Petre C, Vanhoenacker FM. Breast augmentation by injection of free silicone: MRI findings. JBR-BTR. 2012;95:34. https://doi.org/10.5334/jbr-btr.568
- Carson B, Cox S, Ismael H. Giant siliconoma mimicking locally advanced breast cancer: A case report and review of literature. Int J Surg Case Rep. 2018;48:54-60. doi:10.1016/j.ijscr.2018.05.001 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6028662
- Update on the Safety of Silicone Gel-Filled Breast Implants (2011) – Executive Summary. https://www.fda.gov/medical-devices/breast-implants/update-safety-silicone-gel-filled-breast-implants-2011-executive-summary
- Types of Breast Implants. https://www.fda.gov/medical-devices/breast-implants/types-breast-implants
- Nakahori R, Takahashi R, Akashi M, Tsutsui K, Harada S, Matsubayashi RN, Nakagawa S, Momosaki S, Akagi Y. Breast carcinoma originating from a silicone granuloma: a case report. World J Surg Oncol. 2015 Feb 22;13:72. doi: 10.1186/s12957-015-0509-6
- Rupani A, Frame JD, Kamel D. Lymphomas Associated with Breast Implants: A Review of the Literature. Aesthet Surg J. 2015 Jul;35(5):533-44. doi: 10.1093/asj/sjv016
- Takenaka M, Tanaka M, Isobe M, Yamaguchi R, Kojiro M, Shirouzu K. Angiosarcoma of the breast with silicone granuloma: A case report. Kurume Med J. 2009;56:33–37. https://doi.org/10.2739/kurumemedj.56.33
- Bondurant S, Ernster V, Herdman R. Antinuclear antibodies and silicone breast implants. In: Safety of Silikon Breast Implants. Washington: The National Academy Press; 1999. pp. 198-214.
- Lemperle G, Morhenn V, Charrier U. Human histology and persistence of various injectable filler substances for soft tissue augmentation. Aesthetic Plastic Surgery. 2003;27:354-366. DOI: 10.1007/s00266-003-3022-1
- Harlim A, Kanoko M, Aisah S. Classification of foreign body reaction due to industrial silicone injection. Dermatologic Surgery. 2018;9(44):1174-1182
- Harlim A, Kanoko M, Aisah S. Classification of Foreign Body Reactions due to Industrial Silicone Injection. Dermatol Surg. 2018 Sep;44(9):1174-1182. doi: 10.1097/DSS.0000000000001531
- Guttman C Silicone granuloma management: TNF inhibitors may be effective as intervention Dermatol Times May2003;75- 76.
- Utz JP, Limper AH, Kalra S, Specks U, Scott JP, Vuk-Pavlovic Z, Schroeder DR. Etanercept for the treatment of stage II and III progressive pulmonary sarcoidosis. Chest. 2003 Jul;124(1):177-85. doi: 10.1378/chest.124.1.177
- Khanna D, Liebling MR, Louie JS. Etanercept ameliorates sarcoidosis arthritis and skin disease. J Rheumatol. 2003 Aug;30(8):1864-7.
- Hayes MK, Gold RH, Bassett LW. Mammographies findings after the removal of breast implants. AJR Am J Roentgenol. 1993;160:487–490. https://doi.org/10.2214/ajr.160.3.8430541
- Grubstein A, Cohen M, Steinmetz A, Cohen D. Siliconomas mimicking cancer. Clin Imaging. 2011 May-Jun;35(3):228-31. doi: 10.1016/j.clinimag.2010.07.006
- Liu S, Lim AA. Evaluation and treatment of surgical management of silicone mastitis. J Cutan Aesthet Surg. 2012 Jul;5(3):193-6. doi: 10.4103/0974-2077.101380
- Harris KM, Ganott MA, Shestak KC, Losken HW, Tobon H. Silicone implant rupture: detection with US. Radiology. 1993;187:761–768. https://doi.org/10.1148/radiology.187.3.8497626
- Chuangsuwanich A, Warnnissorn M, Lohsiriwat V. Siliconoma of the breasts. Gland Surg. 2013 Feb;2(1):46-9. doi: 10.3978/j.issn.2227-684X.2013.02.05
- Kao CC, Rand RP, Holt CA, Pierce RH, Timmons JH, Wood DE. Internal mammary silicone lymphadenopathy mimicking recurrent breast cancer. Plast Reconstr Surg. 1997 Jan;99(1):225-9. doi: 10.1097/00006534-199701000-00034
- Senet P, Bachelez H, Ollivaud L, Vignon-Pennamen D, Dubertret L. Minocycline for the treatment of cutaneous silicone granulomas. Br J Dermatol. 1999 May;140(5):985-7. doi: 10.1046/j.1365-2133.1999.02853.x





{kind=link}