Transposition of the great arteries
Transposition of the great arteries (TGA) also called dextro-transposition of the great arteries (D-TGA), is a serious but rare heart defect that occurs from birth (congenital), in which the two major arteries that carry blood away from the heart, the aorta and the pulmonary artery, are switched in position or “transposed”. A rarer type of transposition of the great arteries is called levo-transposition of the great arteries (L-TGA).
The Centers for Disease Control and Prevention (CDC) estimates that about 1,153 babies are born with transposition of the great arteries each year in the United States 1. This means that every 1 in 3,413 babies born in the US is affected by transposition of the great arteries.
Transposition of the great arteries changes the way blood circulates through the body, leaving a shortage of oxygen in blood flowing from the heart to the rest of the body. Without an adequate supply of oxygen-rich blood, the body can’t function properly and your child faces serious complications or death without treatment.
Transposition of the great arteries is usually detected either prenatally or within the first hours to weeks of life.
The cause of transposition of the great arteries is unknown. It is not associated with any one common genetic abnormality. It rarely occurs in other family members.
Transposition of the great arteries is a cyanotic heart defect. This means there is decreased oxygen in the blood that is pumped from the heart to the rest of the body.
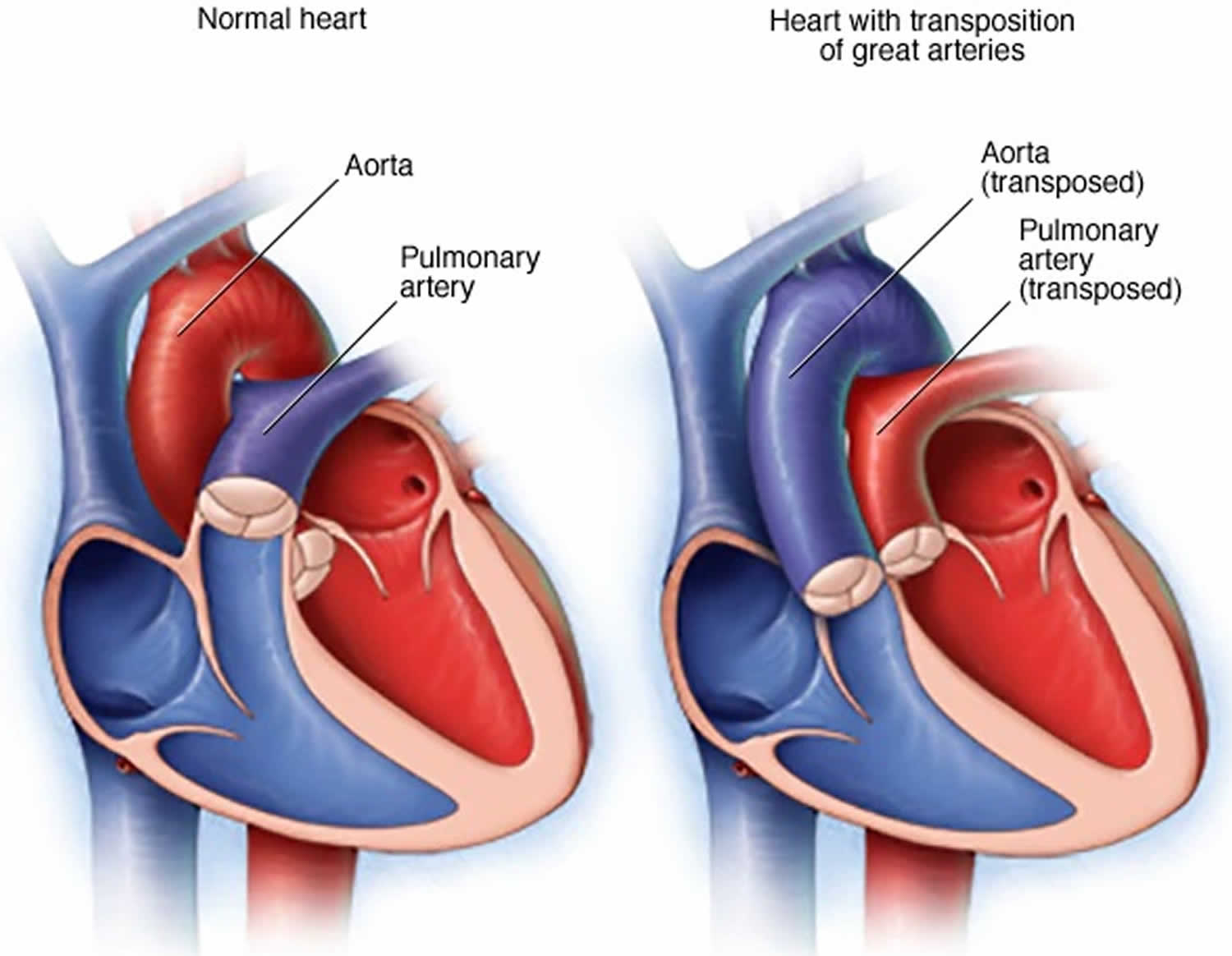
In normal hearts, blood that returns from the body goes through the right side of the heart and pulmonary artery to the lungs to get oxygen. The blood then comes back to the left side of the heart and travels out the aorta to the body.
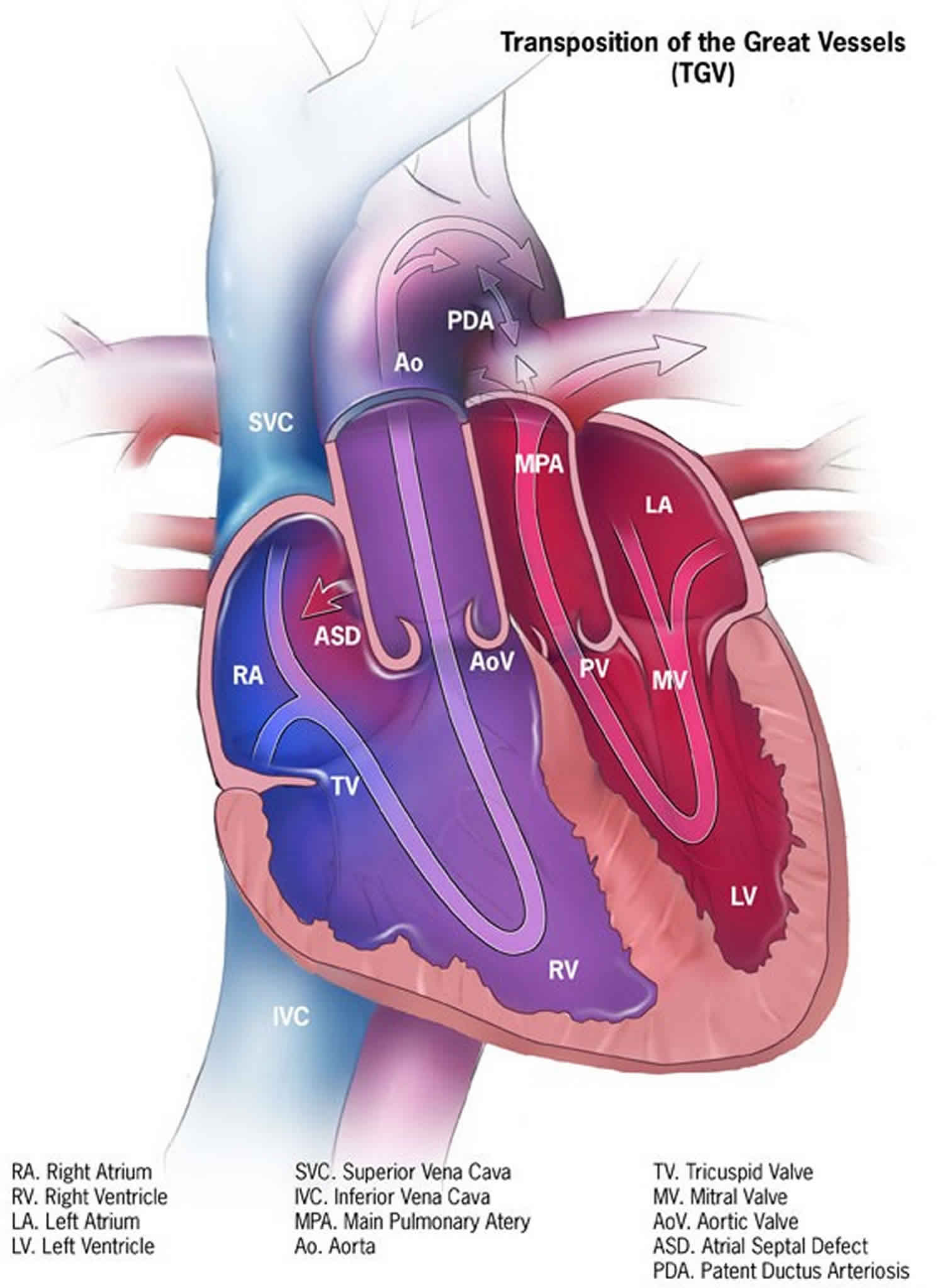
In transposition of the great arteries, venous blood returns normally to the heart through the right atrium. But, instead of going to the lungs to absorb oxygen, this blood is pumped out through the aorta and back to the body. This blood has not been recharged with oxygen and leads to cyanosis.
Symptoms appear at birth or very soon afterward. How bad the symptoms are depends on the type and size of additional heart defects (such as atrial septal defect, ventricular septal defect, or patent ductus arteriosus) and how much the blood can mix between the two abnormal circulations.
Corrective surgery soon after birth is the usual treatment for transposition of the great arteries. Having a baby with transposition of the great arteries can be alarming, but with proper treatment, the outlook is promising.
The initial step in treatment is to allow oxygen-rich blood to mix with poorly oxygenated blood. The baby will immediately receive a medicine called prostaglandin through an IV (intravenous line). This medicine helps keep a blood vessel called the ductus arteriosus open, allowing some mixing of the two blood circulations. In some cases, an opening between the right and left atrium can be created with procedure using a balloon catheter. This allows blood to mix. This procedure is known as balloon atrial septostomy.
Permanent treatment involves heart surgery during which the great arteries are cut and stitched back to their correct position. This is called an arterial switch operation (ASO). Prior to the development of this surgery, a surgery called an atrial switch (or Mustard procedure or Senning procedure) was used.
Figure 1. Transposition of the great arteries
Transposition of the great arteries is often detected as soon as your baby is born or during the first week of life.
If signs and symptoms didn’t appear in the hospital, seek emergency medical help if you notice that your baby develops bluish discoloration of the skin (cyanosis), especially involving the face and body.
Levo-transposition of the great arteries
In this rare type of transposition of the great arteries called levo-transposition of the great arteries or sometimes referred to as congenitally corrected transposition — the two ventricles are switched so that the left ventricle is on the heart’s right side and receives blood from the right atrium, and the right ventricle is on the heart’s left side and receives blood from the left atrium. This type of transposition of the great arteries is sometimes also called congenitally corrected transposition.
However, the blood usually circulates correctly through the heart and body. The right-sided left ventricle attaches to the pulmonary artery, which delivers oxygen-poor blood to the lungs, while the left-sided right ventricle attaches to the aorta, which carries oxygen-rich blood to the body.
Because the circulation is congenitally corrected, some people with this rare condition may not experience symptoms for many years and go undiagnosed until adulthood. However, many people with this condition have other congenital heart defects that may cause symptoms, and these people are usually found to have heart disease as children. Depending on their condition and heart defects, people may have surgery to repair the defects.
The right ventricle may not function well as the main pumping chamber over time, which can lead to heart failure in adults. Adults often also have abnormal function of the valve guarding the right ventricle (tricuspid valve). Abnormal valve and ventricular function can cause heart failure. Treatment such as valve replacement, ventricular assist devices or a heart transplant may eventually be needed.
Transposition of the great arteries causes
Transposition of the great arteries occurs during fetal growth when your baby’s heart is developing. Why this defect occurs is unknown in most cases.
Normally, the pulmonary artery — which carries blood from your heart to your lungs to receive oxygen — is attached to the lower right chamber (right ventricle).
From your lungs, the oxygen-rich blood goes to your heart’s upper left chamber (left atrium), through the mitral valve into the lower left chamber (left ventricle). The aorta is normally attached to the left ventricle. It carries oxygen-rich blood out of your heart back to the rest of your body.
In transposition of the great arteries, the positions of the pulmonary artery and the aorta are switched. The pulmonary artery is connected to the left ventricle, and the aorta is connected to the right ventricle.
Oxygen-poor blood circulates through the right side of the heart and back to the body without passing through the lungs. Oxygen-rich blood circulates through the left side of the heart and directly back into the lungs without being circulated to the rest of the body.
Circulation of oxygen-poor blood through the body causes the skin to have a blue tint (cyanosis). Because of this, transposition of the great arteries is called a cyanotic congenital heart defect.
Although some factors, such as genetics, rubella or other viral illnesses during pregnancy, maternal age over 40, or maternal diabetes, may increase the risk of this condition, in most cases the cause is unknown.
Risk factors for transposition of the great arteries
Although the exact cause of transposition of the great arteries is unknown, several factors may increase the risk of a baby being born with this condition, including:
- A history of German measles (rubella) or another viral illness in the mother during pregnancy
- Drinking alcohol during pregnancy
- Smoking during pregnancy
- Poorly controlled diabetes during pregnancy or a mother who has poorly controlled diabetes
- Mother who is over 40 years old
- Family history of transposition of the great arteries or other congenital heart defects
- Poor nutrition during pregnancy.
Transposition of the great arteries prevention
In most cases, transposition of the great arteries can’t be prevented. If you have a family history of heart defects or if you already have a child with a congenital heart defect, consider talking with a genetic counselor and a cardiologist experienced in congenital heart defects before getting pregnant.
Women who plan to become pregnant should be immunized against rubella if they are not already immune.
Additionally, it’s important to take steps to have a healthy pregnancy. For example, before becoming pregnant, be sure you’re up to date on all of your immunizations, and start taking a multivitamin with 400 micrograms of folic acid.
Eating well, avoiding alcohol, and controlling diabetes both before and during pregnancy may be helpful.
Transposition of the great arteries symptoms
Transposition of the great arteries symptoms include:
- Blue color of the skin (cyanosis)
- Shortness of breath
- Lack of appetite
- Poor feeding
- Clubbing of the fingers or toes
- Poor weight gain.
Transposition of the great arteries complications
Potential complications of transposition of the great arteries include:
- Lack of oxygen to tissues. Your baby’s tissues will receive too little oxygen (hypoxia). Unless there’s some mixing of oxygen-rich blood and oxygen-poor blood within your baby’s body, he or she won’t be able to survive.
- Coronary artery problems
- Heart valve problems
- Irregular heart rhythms (arrhythmias)
- Heart failure. Heart failure — a condition in which the heart can’t pump enough blood to meet the body’s needs — may develop over time because the right ventricle is pumping under higher pressure than usual. This added stress may make the muscle of the right ventricle stiff or weak.
- Lung damage. Too much oxygen-rich blood can cause damage to the lungs, making breathing difficult.
Surgery is required for all babies with transposition of the great arteries early in life, usually within the first week. The most common type of surgery to correct transposition when identified in babies is the arterial switch operation. During this operation, the surgeon moves the great arteries so they are connected to the correct pumping chamber. The arteries that supply the heart (coronary arteries) must also be moved. Although this operation is lifesaving, problems may occur later in life, including:
- Narrowing of the arteries that supply blood to the heart (coronary arteries)
- Heart rhythm abnormalities (arrhythmias)
- Heart muscle weakness or stiffness leading to heart failure
- Narrowed connections where the great vessels are connected
- Leaky heart valves
Transposition of the great arteries diagnosis
Although it’s possible your baby’s transposition of the great arteries may be diagnosed before birth, it can be difficult to diagnose. Prenatal tests for transposition of the great arteries aren’t usually done unless your doctor suspects your baby may have congenital heart disease.
After your baby is born, his or her doctor will immediately suspect a heart defect such as transposition of the great arteries if your baby has blue-tinged skin (cyanosis) or if your baby is having trouble breathing. The health care provider may detect a heart murmur while listening to the chest with a stethoscope.
Sometimes, the bluish skin color isn’t as noticeable if your baby has another heart defect, such as a hole in the wall separating the left and right chambers of the heart (septum), that’s allowing some oxygen-rich blood to travel through the body. If the hole is in the upper chambers of the heart, it’s called an atrial septal defect (ASD). In the lower chambers of the heart, the defect is called a ventricular septal defect (VSD).
It’s also possible your baby could have a patent ductus arteriosus (PDA) — an opening between the heart’s two major blood vessels, the aorta and the pulmonary artery — that allows oxygen-rich and oxygen-poor blood to mix.
As your baby becomes more active, the heart defects won’t allow enough blood through and eventually the cyanosis will become obvious.
Your baby’s doctor may also suspect a heart defect if he or she hears a heart murmur — an abnormal whooshing sound caused by turbulent blood flow.
A physical exam alone isn’t enough to accurately diagnose transposition of the great arteries. One or more of the following tests are necessary for an accurate diagnosis:
- Pulse oximetry (to check blood oxygen level)
- Echocardiogram. An echocardiogram is an ultrasound of the heart — it uses sound waves that bounce off your baby’s heart and produce moving images that can be viewed on a video screen (if done before birth, it is called a fetal echocardiogram). Doctors use this test to diagnose transposition of the great arteries by looking at the position of the aorta and the pulmonary artery. Echocardiograms can also identify associated heart defects, such as a ventricular septal defect, atrial septal defect or patent ductus arteriosus.
- Cardiac catheterization. This procedure is typically done only when other tests, such as an echocardiogram, don’t show enough information to make a diagnosis. During a cardiac catheterization, the doctor inserts a thin flexible tube (catheter) into an artery or vein in your baby’s groin and directs it up to his or her heart. A dye is injected through the catheter to make your baby’s heart structures visible on X-ray pictures. The catheter also measures pressure in the chambers of your baby’s heart and in the blood vessels and can measure the amount of oxygen in the blood. Cardiac catheterization may be done urgently to perform a temporary treatment for transposition of the great arteries (balloon atrial septostomy).
- Chest X-ray. Although a chest X-ray doesn’t provide a definitive diagnosis of transposition of the great arteries, it does allow the doctor to see your baby’s heart size and the position of the aorta and pulmonary artery.
- Electrocardiogram (ECG). An electrocardiogram records the electrical activity in the heart each time it contracts. During this procedure, patches with wires (electrodes) are placed on your baby’s chest, wrists and ankles. The electrodes measure electrical activity, which is recorded on paper.
Transposition of the great arteries treatment
All infants with transposition of the great arteries need surgery to correct the defect.
Before surgery
Your baby’s doctor may recommend several options to help manage the condition before corrective surgery. They include:
- Medication. The medication prostaglandin E1 (alprostadil) helps keep the connection between the aorta and pulmonary artery open (ductus arteriosus), increasing blood flow and improving mixing of oxygen-poor and oxygen-rich blood until surgery can be performed.
- Atrial septostomy. This procedure — usually done using cardiac catheterization rather than surgery — enlarges a natural connection between the heart’s upper chambers (atria). It allows for the oxygen-rich and oxygen-poor blood to mix and results in improved oxygen delivery to your baby’s body.
Surgery
Surgical options include:
Arterial switch operation
This is the most common surgery used to correct transposition of the great arteries. Surgeons usually perform this surgery within the first month of life. It restores usual blood flow through the heart and out to the rest of the body.
During an arterial switch operation, the pulmonary artery and the aorta are moved to their normal positions: The pulmonary artery is connected to the right ventricle, and the aorta is connected to the left ventricle. The coronary arteries (small arteries that provide blood to the heart muscle) also must be moved and reattached to the aorta.
If your baby has a ventricular septal defect or an atrial septal defect, those holes usually are closed during surgery. In some cases, however, the doctor may leave small ventricular septal defects to close on their own.
Atrial switch operation
Atrial switch procedure is less commonly performed. In this surgery, the arteries are left in place, but a tunnel (baffle) is created between the heart’s two upper chambers (atria). This diverts the oxygen-poor blood to the left ventricle and the pulmonary artery and the oxygen-rich blood to the right ventricle and the aorta. This tunnel allows oxygen-poor blood to move from the right atrium to the left ventricle and out the pulmonary artery to the lungs. Returning oxygen-rich blood moves through the tunnel from the left atrium to the right ventricle and out the aorta to the body. Although this repair helps blood to go to the lungs and then out to the body, it also makes extra work for the right ventricle to pump blood to the entire body. Therefore, this repair can lead to difficulties later in life.
With this procedure, the right ventricle must pump blood to the body, instead of just to the lungs as it would do in a normal heart. Possible complications of the atrial switch operation include irregular heartbeats, baffle obstructions or leaks, and heart failure due to long-term problems with right ventricle function.
After surgery
Infants who have these surgeries are not cured; they may have lifelong complications. After corrective surgery, your baby will need lifelong follow-up care with a heart doctor (cardiologist) who specializes in congenital heart disease to monitor his or her heart health and avoid complications or other health problems. The cardiologist may recommend that your child avoid certain activities, such as weightlifting or competitive sports, because they raise blood pressure and may stress the heart.
Talk to your or your child’s doctor about what type of physical activities you or your child can do, and how much and how often.
Many people who undergo the arterial switch operation don’t need additional surgery. However, some complications, such as arrhythmias, heart valve leaks or problems with the heart’s pumping, may require additional treatment.
After surgery, medications may also be needed to help the heart pump better, control blood pressure, help get rid of extra fluid in the body, and slow down the heart if it is beating too fast. If the heart is beating too slowly, a pacemaker can be used.
With proper treatment, most babies with d-transposition of the great arteries grow up to lead healthy, productive lives.
Recovery
Expected hospital stay after the arterial switch operation is approximately 2 weeks. This can vary depending on how sick the baby is prior to surgery, time to full feeds postoperatively, and any other issues that may delay discharge.
After surgery, your baby will require continued follow-up care. The doctor will schedule routine checkups to make sure that the procedure was successful and monitor for any new problems. Most children with successful complete repair will not have any activity restrictions as they grow older.
Most children who undergo the arterial switch operation do not need any additional surgery, but sometimes patients who had an operation to repair transposition of the great arteries in infancy need additional surgery as they age.
Most often, this procedure is undertaken to repair or replace leaky heart valves, open up areas of narrowing, abnormal heart rhythm, and address problems with the arteries that supply the heart with blood (coronary arteries).
Long-term care
You or your child will need to be monitored and treated throughout your life. Your child will be monitored and have regular follow-up appointments with a pediatric cardiologist. As your child grows older, his or her care will transition to an adult congenital cardiologist, who can monitor his or her condition over time. Transposition of the great arteries can affect your child’s adult life, as it can contribute to other health problems. Adults who have congenital heart defects may need other treatments for their condition.
Pregnancy
If you had transposition of the great arteries repaired in your infancy, it’s possible for you to have a healthy pregnancy, but specialized care may be necessary. If you’re thinking about becoming pregnant, talk to your cardiologist and obstetrician before conceiving.
If you have complications, such as arrhythmias or serious heart muscle problems, pregnancy may pose risks to both you and your fetus. In some situations, such as for women who have severe complications of their heart defect, pregnancy isn’t recommended even for those with a repaired transposition.
Coping and support
Caring for a baby with a serious heart problem, such as transposition of the great arteries, can be challenging and frightening. Here are some strategies that may help make it easier:
- Seek support. Ask for help from family members and friends. Talk with your child’s cardiologist about support groups and other types of assistance that are available near you.
- Record your or your baby’s health history. You may want to write down your baby’s diagnosis, medications, surgery and other procedures and the dates they were performed, your child’s cardiologist’s name and phone number, and any other important information about your baby’s care. This record will help you recall the care your child has received, and it will be helpful for doctors who are unfamiliar with your baby to understand his or her health history.
- Talk about your concerns. You may worry about the risks of vigorous activity, even after your child has had corrective surgery. Talk with the cardiologist about which activities are safe for your child. If some are off-limits, encourage your child in other pursuits rather than focusing on what he or she can’t do.
If you have other concerns about your child’s health, discuss them with your child’s cardiologist, too.
Although every circumstance is different, remember that due to advances in surgical treatment, most babies with transposition of the great arteries grow up to lead active lives.
Transposition of the great arteries prognosis
The child’s symptoms will improve after surgery to correct the defect. Most infants who undergo arterial switch do not have symptoms after surgery and live normal lives. If corrective surgery is not performed, the life expectancy is only months.
Preventive antibiotics are almost always recommended for people who have artificial valves or who’ve had repair with prosthetic material. Be sure to ask your doctor about what is right for your child.
References




{kind=link}