Trichuriasis
Trichuriasis also known as whipworm infection. The name is derived from the Trichuris trichiura worm’s distinctive whip-like shape. Human whipworm infection or trichuriasis is caused by ingesting eggs. This can happen when hands or fingers that have contaminated dirt on them are put in the mouth or by consuming vegetables or fruits that have not been carefully cooked, washed or peeled. Whipworms (Trichuris trichiura) live in the large intestine and whipworm eggs are passed in the feces of infected persons. If the infected person defecates outside (near bushes, in a garden, or field) or if human feces as used as fertilizer, eggs are deposited on soil. They can then mature into a form that is infective.
Whipworm is a soil-transmitted helminth (helminthiasis) and is the third most common roundworm (nematode) of humans. Trichuriasis or whipworm infection occurs worldwide in warm and humid climates where sanitation and hygiene are poor, including in temperate climates during warmer months and among children. Persons in these areas are at risk if soil contaminated with human feces enters their mouths or if they eat vegetables or fruits that have not been carefully washed, peeled or cooked. In 2002, it is estimated that 1 billion people are infected with whipworm worldwide. Trichuriasis also occurs in the southern United States.
People infected with whipworm can suffer light or heavy infections. People with light infections usually have no symptoms. People with heavy symptoms can experience frequent, painful passage of stool that contains a mixture of mucus, water, and blood. Rectal prolapse can also occur. Children with heavy infections can become severely anemic and growth-retarded. Trichuriasis or whipworm infections are treatable with medication prescribed by your health care provider.
Trichuriasis life cycle
The unembryonated eggs are passed with the stool (number 1). In the soil, the eggs develop into a 2-cell stage (number 2), an advanced cleavage stage (number 3) and then they embryonate (number 4); eggs become infective in 15 to 30 days. After ingestion (soil-contaminated hands or food), the eggs hatch in the small intestine, and release larvae (number 5) that mature and establish themselves as adults in the colon (number 6). The adult worms (approximately 4 cm in length) live in the cecum and ascending colon. The adult worms are fixed in that location, with the anterior portions threaded into the mucosa. The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day. The life span of the adults is about 1 year.
Figure 1. Trichuris trichiura life cycle
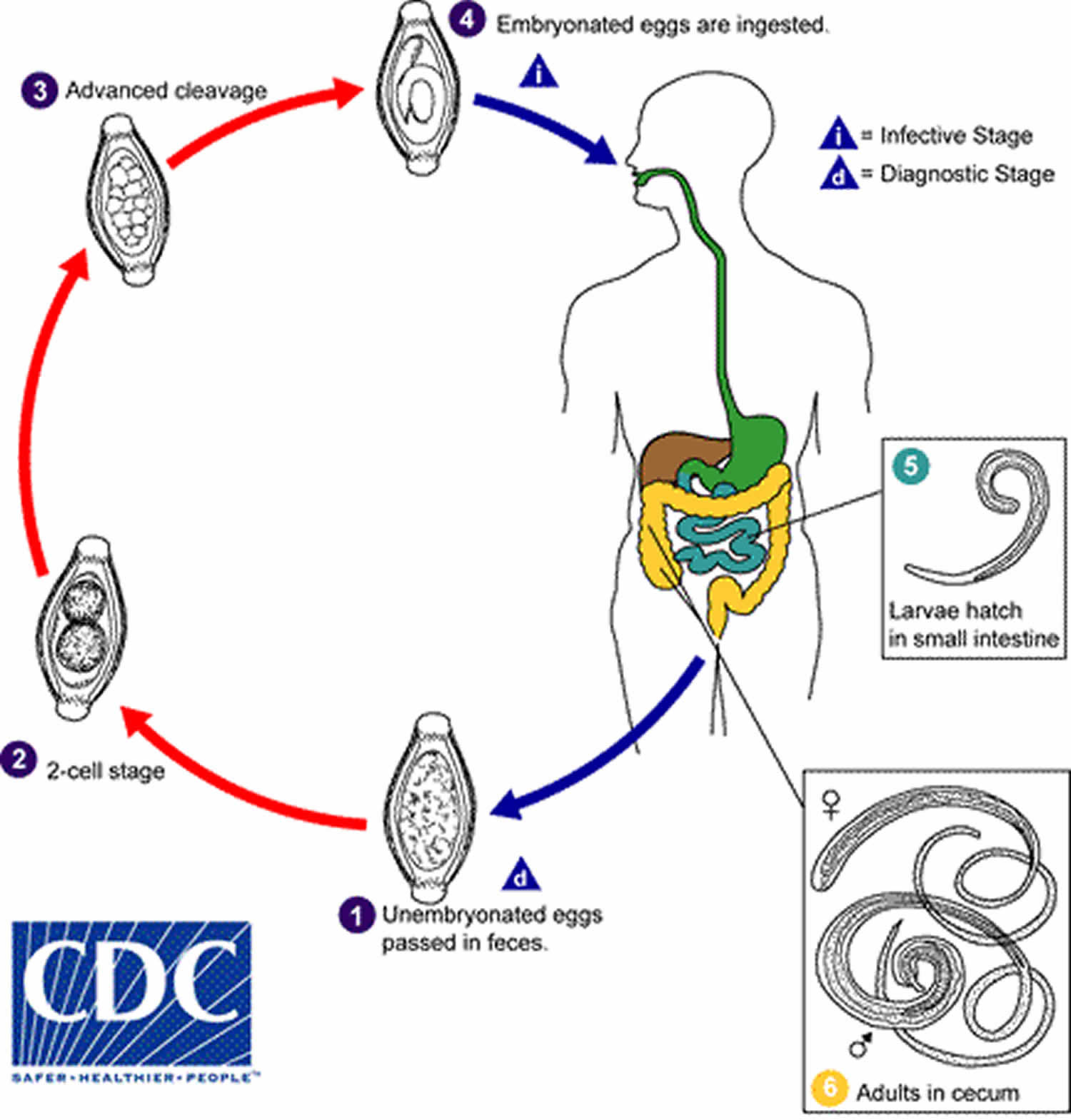 Figure 2. Trichuris trichiura adult worm
Figure 2. Trichuris trichiura adult worm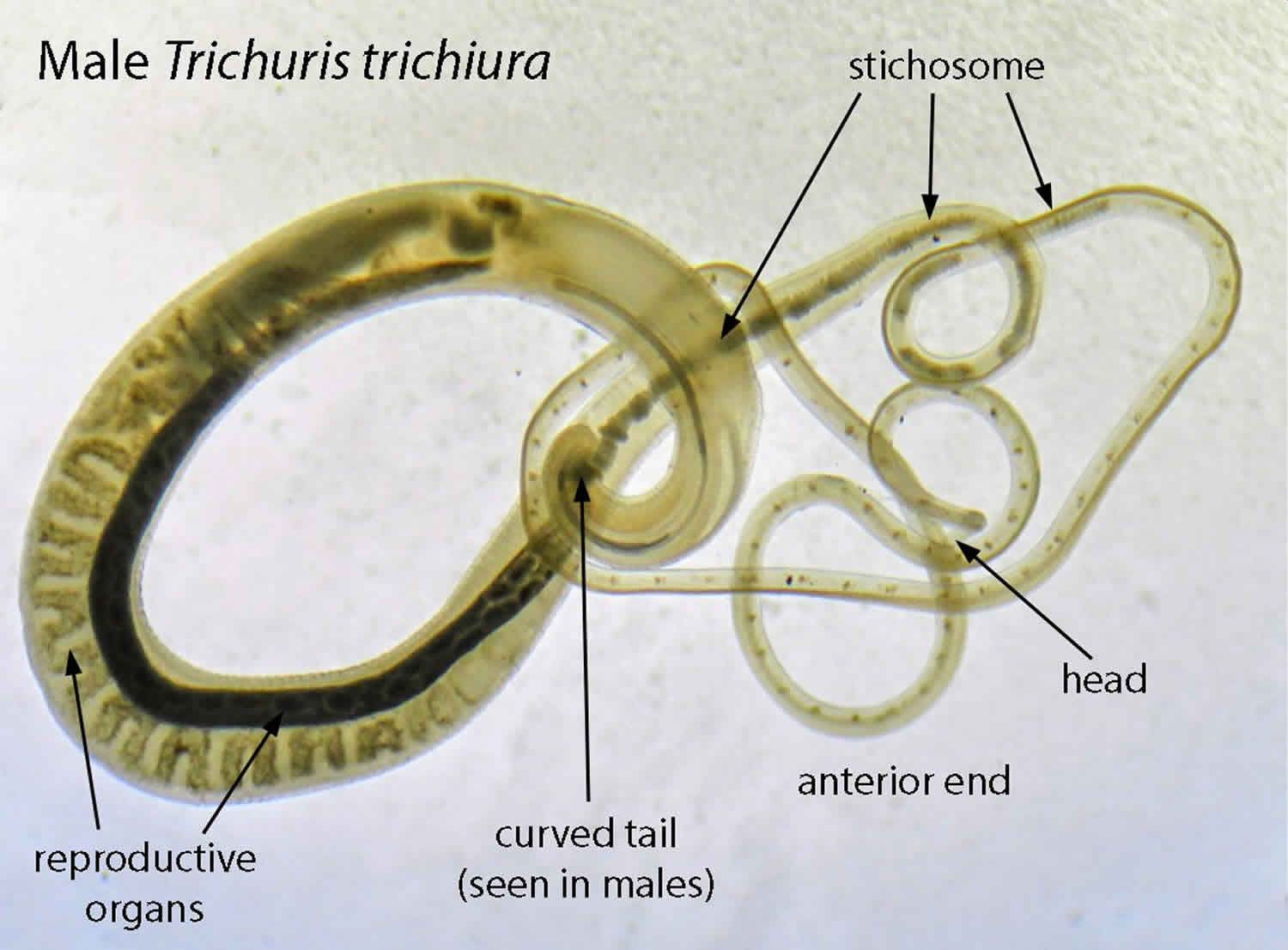
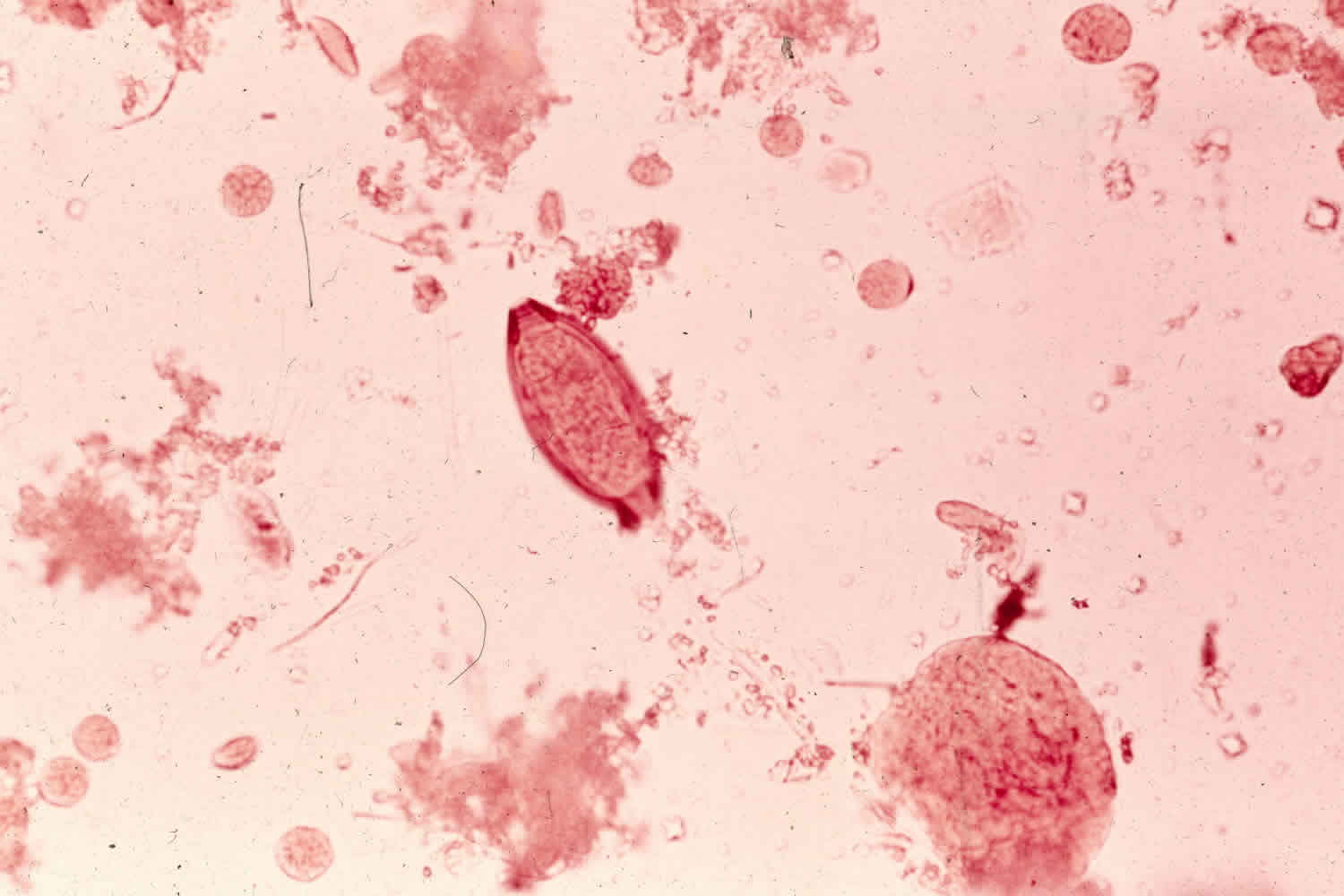
Figure 3. Trichuris trichiura egg (unstained wet mount)

Trichuriasis causes
Whipworms or Trichuris trichiura live in the intestine and whipworm eggs are passed in the feces of infected persons. If the infected person defecates outside (near bushes, in a garden, or field), or if the feces of an infected person are used as fertilizer, then eggs are deposited on the soil. They can then mature into a form that is infective. Roundworm infection is caused by ingesting eggs. This can happen when hands or fingers that have contaminated dirt on them are put in the mouth, or by consuming vegetables or fruits that have not been carefully cooked, washed or peeled.
Trichuriasis prevention
- Avoid contact with soil that may be contaminated with human feces, including with human fecal matter (“night soil”) used to fertilize crops.
- Wash your hands with soap and warm water before handling food.
- Teach children the importance of washing hands to prevent infection.
- Wash, peel, or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with manure.
Transmission of whipworm infection to others can be prevented by:
- not defecating outdoors, and by
- effective sewage disposal systems.
Trichuriasis symptoms
People infected with whipworm can suffer light or heavy infections. People with light whipworm infections usually have no signs or symptoms. People with heavy whipworm infections can experience frequent, painful passage of stool that contains a mixture of mucus, water, and blood. The diarrhea typically has an acrid smell. In severe cases growth retardation can occur. Rectal prolapse can also occur. In children, heavy infection may be associated with growth retardation and impaired cognitive development.
Trichuriasis complications
Trichuris trichiura dysentery syndrome can be found in children (with no adult cases noted) and is seen when there is a very high worm burden. This often leads to diarrhea, tenesmus, iron deficiency anemia and growth retardation. The growth retardation is typically secondary to poor nutrition and consequently causes the cognitive delay.
Trichuriasis diagnosis
Health care providers can diagnose whipworm by taking a stool sample. By using a microscope, providers can look for the presence of whipworm eggs. Because eggs may be difficult to find in light infections, a concentration procedure is recommended. Because the severity of symptoms depend on the worm burden, quantification of the latter (e.g. with the Kato-Katz technique) can prove useful. The diagnosis is made by using the Kato-Katz method for counting eggs per unit weight of feces. One caveat is that from the time the eggs are ingested to development of the mature worm, there is a time lag of about three months. During this period, there may be no signs of an infestation and the stools may not show evidence of any eggs or shedding.
Examination of the rectal mucosa by proctoscopy (or directly in case of prolapses) can occasionally demonstrate adult worms.
There have been case reports of patients reporting symptoms in areas that are resource-rich where the diagnosis has been made with colonoscopy. The classic finding is the “coconut cake rectum.” There have recently been studies which show a whipworm dance on ultrasound, and this is a modality that can easily be used in resource-poor settings 1.
PCR assays are currently being developed and used. This has improved the specificity and sensitivity of detecting the whipworm 2.
Trichuriasis treatment
Whipworm infections are generally treated for 1-3 days with anthelminthic medications (drugs that rid the body of parasitic worms), such as albendazole, mebendazole or ivermectin, prescribed by your health care provider. Dosage guidelines are the same for children as for adults. Albendazole should be taken with food. Ivermectin should be taken with water on an empty stomach and the safety of ivermectin for children weighing less than 15 kg has not been established. Neither albendazole nor ivermectin is FDA-approved for treating whipworm. The drugs are effective and appear to have few side effects. Your health care provider may decide to repeat a stool exam after treatment. Iron supplements may also be prescribed if the infected person suffers from anemia.
| Drug | Dosage for adults and children |
|---|---|
| Albendazole | 400 mg orally for 3 days |
| Mebendazole | 100 mg orally twice a day for 3 days |
| Ivermectin | 200 mcg/kg/day orally for 3 days |
The suggested dose of mebendazole 100 mg twice a day for 3 days or albendazole is 200 to 400 mg twice a day for 3 days. Mebendazole has been shown to be more effective and is considered the first-line treatment.
Ivermectin (200 mcg/kg daily) can be used; however, it is not as effective as the first 2.
It is important to keep in mind that there are often co-infections with other helminths so treatments with multiple medications may be required.
Adults and children should be treated appropriately for the anemia they experience. Many global organizations stress the importance of increased education for children who have been treated for whipworm infection. Not doing so keeps them behind in school when compared to peers of their same age group who were not infected.
Albendazole
Treatment in pregnancy
Albendazole is pregnancy category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Data on the use of albendazole in pregnant women are limited, though the available evidence suggests no difference in congenital abnormalities in the children of women who were accidentally treated with albendazole during mass prevention campaigns compared with those who were not. In mass prevention campaigns for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of albendazole in the 2nd and 3rd trimesters of pregnancy. However, the risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Treatment during lactation
It is not known whether albendazole is excreted in human milk. Albendazole should be used with caution in breastfeeding women.
Treatment in children
The safety of albendazole in children less than 6 years old is not certain. Studies of the use of albendazole in children as young as one year old suggest that its use is safe. According to WHO guidelines for mass prevention campaigns, albendazole can be used in children as young as 1 year old. Many children less than 6 years old have been treated in these campaigns with albendazole, albeit at a reduced dose.
Mebendazole
Treatment in pregnancy
Albendazole is pregnancy category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Data on the use of mebendazole in pregnant women are limited. The available evidence suggests no difference in congenital anomalies in the children of women who were treated with mebendazole during mass treatment programs compared with those who were not. In mass treatment programs for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of mebendazole in the 2nd and 3rd trimesters of pregnancy. The risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Treatment during lactation
It is not known whether mebendazole is excreted in breast milk. The World Health Organization (WHO) classifies mebendazole as compatible with breastfeeding and allows the use of mebendazole in lactating women.
Treatment in children
The safety of mebendazole in children has not been established. There is limited data in children age 2 years and younger. Mebendazole is listed as an intestinal antihelminthic medicine on the WHO Model List of Essential Medicines for Children, intended for the use of children up to 12 years of age.
Ivermectin
Treatment in pregnancy
Albendazole is pregnancy category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Data on the use of ivermectin in pregnant women are limited, though the available evidence suggests no difference in congenital abnormalities in the children of women who were accidentally treated during mass prevention campaigns with ivermectin compared with those who were not. The World Health Organization (WHO) excludes pregnant women from mass prevention campaigns that use ivermectin. However, the risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Treatment during lactation
Ivermectin is excreted in low concentrations in human milk. Ivermectin should be used in breast-feeding women only when the risk to the infant is outweighed by the risk of disease progress in the mother in the absence of treatment.
Treatment in children
The safety of ivermectin in children who weigh less than 15kg has not been demonstrated. According to the WHO guidelines for mass prevention campaigns, children who are at least 90 cm tall can be treated safely with ivermectin. The WHO growth standard curves show that this height is reached by 50% of boys by the time they are 28 months old and by 50% of girls by the time they are 30 months old, many children less than 3 years old been safely treated with ivermectin in mass prevention campaigns, albeit at a reduced dose.
Trichuriasis prognosis
Trichuris trichiura whipworm tends to be more resistant to treatment than other helminths, with some studies listing cure rates as low as 28% to 36%. Trichuris trichiura whipworms can still be present after treatment however it is thought that a low worm count leads to no significant disease burden.
References- Vijayaraghavan SB. Sonographic whipworm dance in trichuriasis. J Ultrasound Med. 2009 Apr;28(4):555-6.
- Pilotte N, Papaiakovou M, Grant JR, Bierwert LA, Llewellyn S, McCarthy JS, Williams SA. Improved PCR-Based Detection of Soil Transmitted Helminth Infections Using a Next-Generation Sequencing Approach to Assay Design. PLoS Negl Trop Dis. 2016 Mar;10(3):e0004578





{kind=link}