Trigonitis
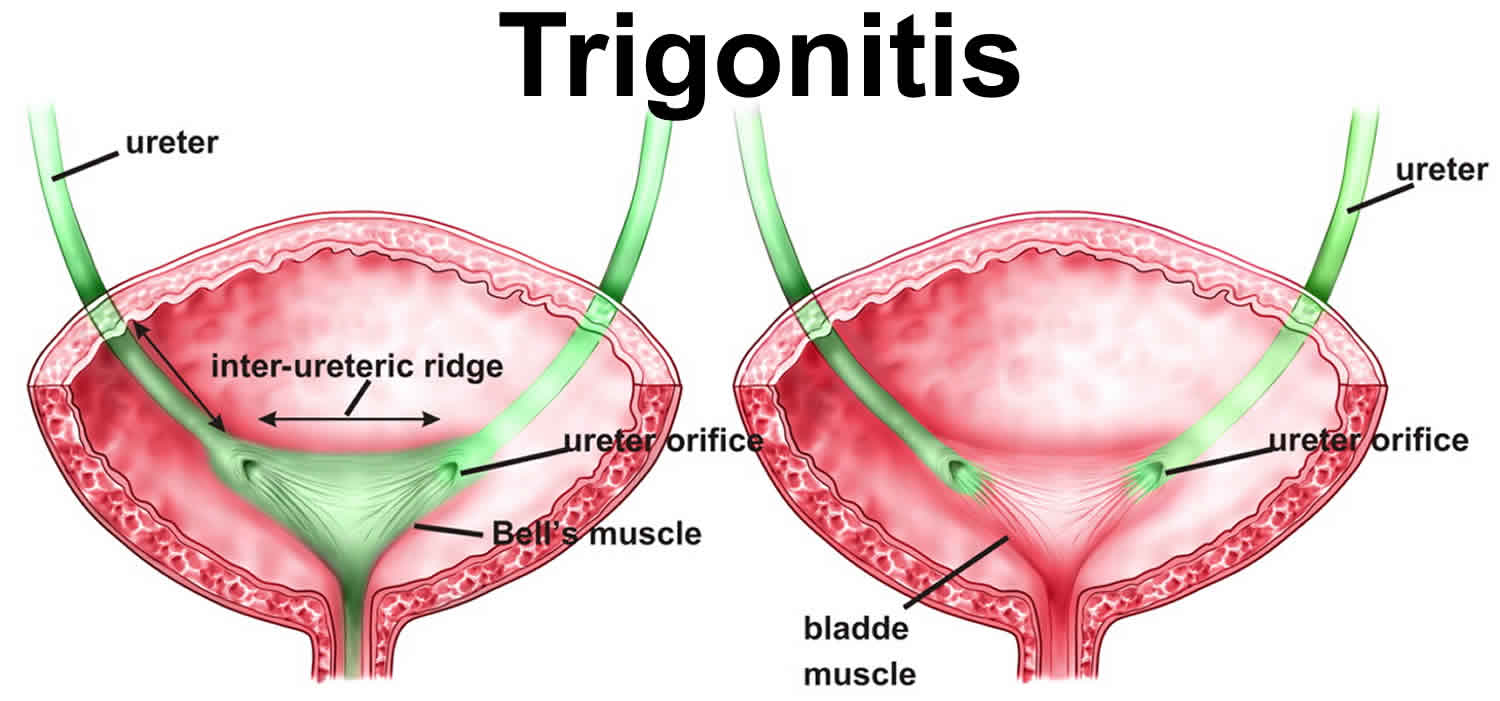
Trigonitis refers to the nonkeratinizing squamous metaplastic changes in the bladder trigone 1. The trigone is the triangular area of the bladder bound by the ureteral orifices and the internal urethral sphincter, which is normally lined by urothelium, a type of transitional epithelial tissue 2.
Squamous metaplasia of the trigone occurs almost exclusively in women of childbearing age 3. It is almost nonexistent in children. Although the exact cause of trigonitis is unknown, the condition usually occurs in response to an irritative (eg, chronic indwelling catheter) or infectious process 3.
Trigonitis is a benign lesion without malignant potential. Trigonitis does not require follow-up cystoscopy. However, trigonitis should be distinguished from keratinizing squamous metaplasia (leukoplakia), which does require follow-up.
Trigonitis causes
The precise underlying cause of trigonitis is not known, squamous metaplasia in the bladder usually occurs in response to an irritative (eg, chronic indwelling catheter) or infectious process 3.
Because nonkeratinizing squamous metaplasia is most commonly found in adult women of childbearing age, a hormonal influence is posited. In a study of bladder biopsies performed in women with pseudomembranous trigonitis and women who underwent cystoscopy for staging gynecological cancer, estrogen and progesterone receptors were found in the trigone in association with squamous metaplastic changes 4. In a more extensive mapping of estrogen and progesterone receptors in the female lower urinary tract, both were found in squamous epithelial tissue, including the transitional cell epithelium in the trigone and proximal urethra that has undergone squamous metaplastic change 5.
In the first known case report of a 16-year-old boy with Klinefelter syndrome diagnosed with pseudomembranous trigonitis, the findings of raised estrogen levels in conjunction with increased expression of estrogen receptors in the trigone area of the biopsy suggest that estrogen could be an etiological driver, much like the association of Klinefelter syndrome with estrogen-driven cancers such as breast cancer 6.
However, whether hormonal influences lead to squamous metaplasia is unclear. Others have suggested that squamous cell metaplasia is not associated with increased estrogen activity 7. Kvist et al 8 did not find estrogen receptors in 36 historically collected samples of squamous metaplasia of the bladder urothelium, although the authors posited that relatively few existing receptors might have been destroyed in the tissue preparation process.
Instead, other explanations focus on the potential role of chronic inflammation and/or a deficient urothelium. In one autopsy study of adult women, histological evidence of chronic inflammation was found significantly more often in bladders with squamous metaplasia. The authors suggest that squamous metaplasia is not a consequence of chronic inflammation but rather that its surface characteristics may predispose to chronic infection 9.
Squamous metaplasia is observed over edematous or inflamed lamina propria 10. Electron microscopy of the keratinizing variant has demonstrated that squamous metaplastic cells lack the tight junctions seen in normal transitional epithelial cells, which might allow urine to permeate the subepithelial layers and result in ongoing inflammation 11.
Bacterial cystitis has been associated with the development of trigonitis in cases of recurrent urinary tract infections. The interstitial cystitis literature suggests that the mucosal coating of the bladder surface, also known as the glycosaminoglycan (GAG) layer, plays an important role in preventing the permeability of urinary solutes into the bladder wall 12. Restriction of the characteristic lesion to the trigone of the bladder is possibly due to the estrogenic effect. This could be explained by the fact that the trigone is anatomically and embryologically distinct from the remainder of the bladder, thereby allowing the trigonal epithelium to respond to estrogenic stimulation 13.
Defects in this protective mechanism, or injuries resulting from chronic irritation or recurrent infections, may result in chronic inflammatory changes leading to metaplasia. However, not all individuals with squamous metaplasia are symptomatic, and not all symptomatic patients have squamous metaplasia.
Trigonitis symptoms
Individuals with trigonitis (squamous metaplastic changes in the bladder) may be asymptomatic or present with irritative voiding symptoms (eg, frequency, urgency, dysuria), recurrent urinary tract infections (UTIs), hematuria, or pelvic pain. Specific attention should be directed at establishing the presence and pattern of specific voiding symptoms.
Because trigonitis is a cystoscopic finding, a physical examination is unlikely to identify this lesion. However, a complete genitourinary exam may be helpful in ruling out other causes of symptoms that bring the patient to medical attention.
Trigonitis diagnosis
Cystoscopy is necessary to make the diagnosis of trigonitis. Urinalysis and urine culture can be performed to exclude infection, as is often done prior to cystoscopy. Imaging studies are not necessary to confirm the diagnosis. Usually recognized by its distinct gross appearance and typical location in the trigone, biopsy of the lesion is usually deferred. However, biopsy may be warranted in males, females with hematuria, pediatric patients, or if the lesion is outside of the trigone because such lesions are more likely to be keratinizing and potentially precancerous.
In one study of transabdominal ultrasonography, women with asymptomatic, cystoscopically-confirmed trigonitis had thickening of the muscosa around the bladder neck when compared with women who had cystoscopically normal bladders 14.
Histologic findings
Nonkeratinizing squamous metaplasia of the trigone is composed of stratified squamous epithelium that often contains abundant glycogen. The basal cell layer has prominent nuclei with condensed chromatin and nucleoli. The surface cells are linked by desmosomes and are longitudinally oriented. Jost et al found the mitotic index within these lesions to be 0.17%, higher than the expected value of 0% 15.
Trigonitis treatment
Asymptomatic patients do not require treatment. A urologist may be consulted in symptomatic cases. Several treatment approaches have been tried in patients with symptomatic trigonitis, including medications and surgery. Because it presents a constant source of irritation, chronic indwelling instrumentation of the bladder should be discouraged if better alternatives for bladder drainage are feasible.
Treatment with doxycycline proved effective in a study of 103 women with cystoscopially confirmed trigonitis who had presented with persistent urinary frequency, chronic urethral and/or pelvic pain associated with dyspareunia, and/or a history of recurrent urinary tract infections (UTIs) 16. In addition to vaginal tablets to eradicate microbial reservoirs, the women received doxycycline at 100 mg twice daily for 2 weeks, followed by 100 mg daily for 2 weeks. Sexual partners were also treated with doxycycline 100 mg twice daily for 2 weeks, and the use of condoms was recommended during the entire treatment period. Following the treatment, 30% of patients considered themselves cured and 41% reported symptom improvement. On follow-up cystoscopy in 31 patients, trigonitis was completely resolved in 8 cases and diminished in 12 cases 17.
An ongoing randomized trial in Europe is comparing oral clarithromycin 500 mg daily and intravesical sodium hyaluronate instillation at 40 mg weekly (Cystistat) in patients with trigonitis. Sodium hyaluronate is a derivative of hyaluronic acid that replaces the deficient glycosaminoglycan (GAG layer in the bladder wall 18. However, intravesical sodium hyaluronate is not approved by the US Food and Drug Administration (FDA).
Surgical care
Endoscopic treatment with an Nd:YAG laser was attempted in women with urethral syndrome and biopsy-confirmed squamous metaplasia of the bladder refractory to medical treatment. Patients (n=62) were randomized to end-firing or side-firing Nd:YAG laser treatment at 30 W. Although results, as assessed by the Urogenital Distress Inventory short form (UDI-6), were significantly better in the side-firing group, follow-up cystoscopy and biopsy found that squamous metaplastic lesions were no longer present in patients of either group with symptom improvement, but white lesions in the bladder neck and trigone were seen in patients whose symptoms were unchanged or worsened 19.
In a retrospective study of 33 women with longstanding recurrent UTIs refractory to antibiotic treatment who underwent cystoscopy with fulguration of trigonitis, 76% had a complete cystoscopic resolution of the trigonal lesions at 6 months postoperatively. The patients with complete resolution had a significantly decreased need for antibiotic treatment for UTI-related symptoms and/or positive urine cultures compared with the group with residual trigonitis following cystoscopy with fulguration 20.
Trigonitis prognosis
The prognosis for patients with trigonitis (nonkeratinizing squamous metaplasia) of the bladder is excellent.
Trigonitis, or nonkeratinizing squamous metaplasia, is considered benign (non-cancerous) and without malignant potential. However, it must be differentiated from keratinizing squamous metaplasia, also known as leukoplakia, which is characterized by downward growth of rete pegs (acanthosis), cellular atypia, and dysplasia. Leukoplakia is believed to be a response of the normal urothelium to noxious stimuli and is generally considered a premalignant lesion that may progress to squamous cell carcinoma in as many as 20% of cases 2.
References- Jost SP, Gosling JA, Dixon JS. The fine structure of human pseudomembranous trigonitis. British Journal of Urology. 1989;64(5):472–477
- Chai TC, Birder LA. Physiology and Pharmacology of the Bladder and Urethra. Wein AJ, Kavoussi LR, Partin AW, Peters CA, eds. Campbell-Walsh Urology. 11th ed. Philadelphia, PA: Elsevier; 2016. 1631-84.
- Trigonitis. https://emedicine.medscape.com/article/438185-overview
- Pacchioni D, Revelli A, Casetta G, Cassoni P, Piana P, Tizzani A. Immunohistochemical detection of estrogen and progesterone receptors in the normal urinary bladder and in pseudomembranous trigonitis. J Endocrinol Invest. 1992 Nov. 15(10):719-25.
- Blakeman PJ, Hilton P, Bulmer JN. Oestrogen and progesterone receptor expression in the female lower urinary tract, with reference to oestrogen status. BJU Int. 2000 Jul. 86(1):32-8.
- Lian DW, Li FX, Ong CC, Kuick CH, Chang KT. Pseudomembranous trigonitis in a male with Klinefelter syndrome: a case report and evidence of a hormonal etiology. Int J Clin Exp Pathol. 2014 May 26. 7 (6):3375-9.
- Nonkeratinizing Squamous Metaplasia of the Bladder in Children. https://www.medscape.com/viewarticle/447776_2
- Kvist E, Sjølin KE, Laursen H, Orntoft TF, Sturmer MA. Squamous cell metaplasia of the bladder urothelium. A retrospective study of 36 patients. APMIS. 1992 Jul. 100(7):650-4.
- Long ED, Shepherd RT. The incidence and significance of vaginal metaplasia of the bladder trigone in adult women. Br J Urol. 1983 Apr. 55(2):189-94.
- Tannenbaum M. Inflammatory proliferative lesion of urinary bladder: squamous metaplasia. Urology. 1976 Apr. 7(4):428-9.
- Mueller SC, Thueroff JW, Rumpelt HJ. Urothelial leukoplakia: new aspects of etiology and therapy. J Urol. 1987 May. 137(5):979-83.
- Parsons CL. The role of a leaky epithelium and potassium in the generation of bladder symptoms in interstitial cystitis/overactive bladder, urethral syndrome, prostatitis and gynaecological chronic pelvic pain. BJU Int. 2011 Feb. 107(3):370-5.
- Paul S, Singh V, Kumar A, Sankhwar S. Coexistence of inflammatory pseudotumour and pseudomembranous cystitis: a histopathological surprise. BMJ Case Rep. 2014 Jan 6. 2014
- Sugaya K, Nishijima S, Oda M, et al. Transabdominal vesical sonography of urethral syndrome and stress incontinence. Int J Urol. 2003 Jan. 10(1):36-42.
- Jost SP, Gosling JA, Dixon JS. The fine structure of human pseudomembranous trigonitis. Br J Urol. 1989 Nov. 64(5):472-7.
- Burkhard FC, Blick N, Hochreiter WW, Studer UE. Urinary urgency and frequency, and chronic urethral and/or pelvic pain in females. Can doxycycline help? Journal of Urology. 2004;172(1):232–235.
- Burkhard FC, Blick N, Hochreiter WW, Studer UE. Urinary urgency and frequency, and chronic urethral and/or pelvic pain in females. Can doxycycline help?. J Urol. 2004 Jul. 172(1):232-5.
- Stavropoulos M, Papatsoris AG, Konstantinidis C, and Chrisofos M. Pseudomembranous Trigonitis: A Common but Underrecognized Urological Entity. Advances in Urology. 2010.
- Costantini E, Zucchi A, Del Zingaro M, Mearini L. Treatment of urethral syndrome: a prospective randomized study with Nd:YAG laser. Urol Int. 2006. 76(2):134-8.
- Hussain SA, Alhalabi F, and Zimmern PE. Long-term efficacy of fulguration of trigonitis for recurrent urinary tract infections in women. Urol Sci. September 2015. 26(3):197-201.





{kind=link}