
What is X-linked ichthyosis
X-linked recessive ichthyosis also called X-linked ichthyosis, is a genetic disorder in which there is very dry skin that affects males. X-linked recessive ichthyosis features include generalized, fine or rhomboid, adherent, dark brown or light grey, scaling of the skin. The scaling is usually prominent on the back of the neck, upper trunk and extensor surfaces of the limbs. X-linked ichthyosis presents usually at birth or within 6 months of birth.
X-linked recessive ichthyosis is associated with corneal opacities of the eye, undescended testicles and neurological abnormalities.
In X-linked ichthyosis, the skin cells are produced at a normal rate but they do not separate normally at the surface of the stratum corneum (the outermost layer of the skin), and are not shed as quickly as they should be. The result is a build-up of scales. The scales of X-linked ichthyosis are often dark and usually cover only a portion of the body. Typically, the face, scalp, palms of the hands, and soles of the feet are free from scales, while the back of the neck is almost always affected. X-linked ichthyosis frequently improves in the summer. Babies with X-linked ichthyosis often appear normal when they are born, but the skin abnormalities will almost always show up by their first birthday.
Recessive X-linked ichthyosis is an inborn error of metabolism characterized by a deficiency of the enzyme steroid sulfatase (STS). Under normal conditions, this enzyme breaks down (metabolizes) cholesterol sulfate, a member of the chemical family of steroids. Cholesterol sulfate plays a role in maintaining the integrity of the skin. If steroid metabolism is interrupted and cholesterol sulfate accumulates in the skin cells, the skin cells stick together more strongly than usual. The normal shedding of dead skin cells is inhibited and the skin cells build up and clump into scales.
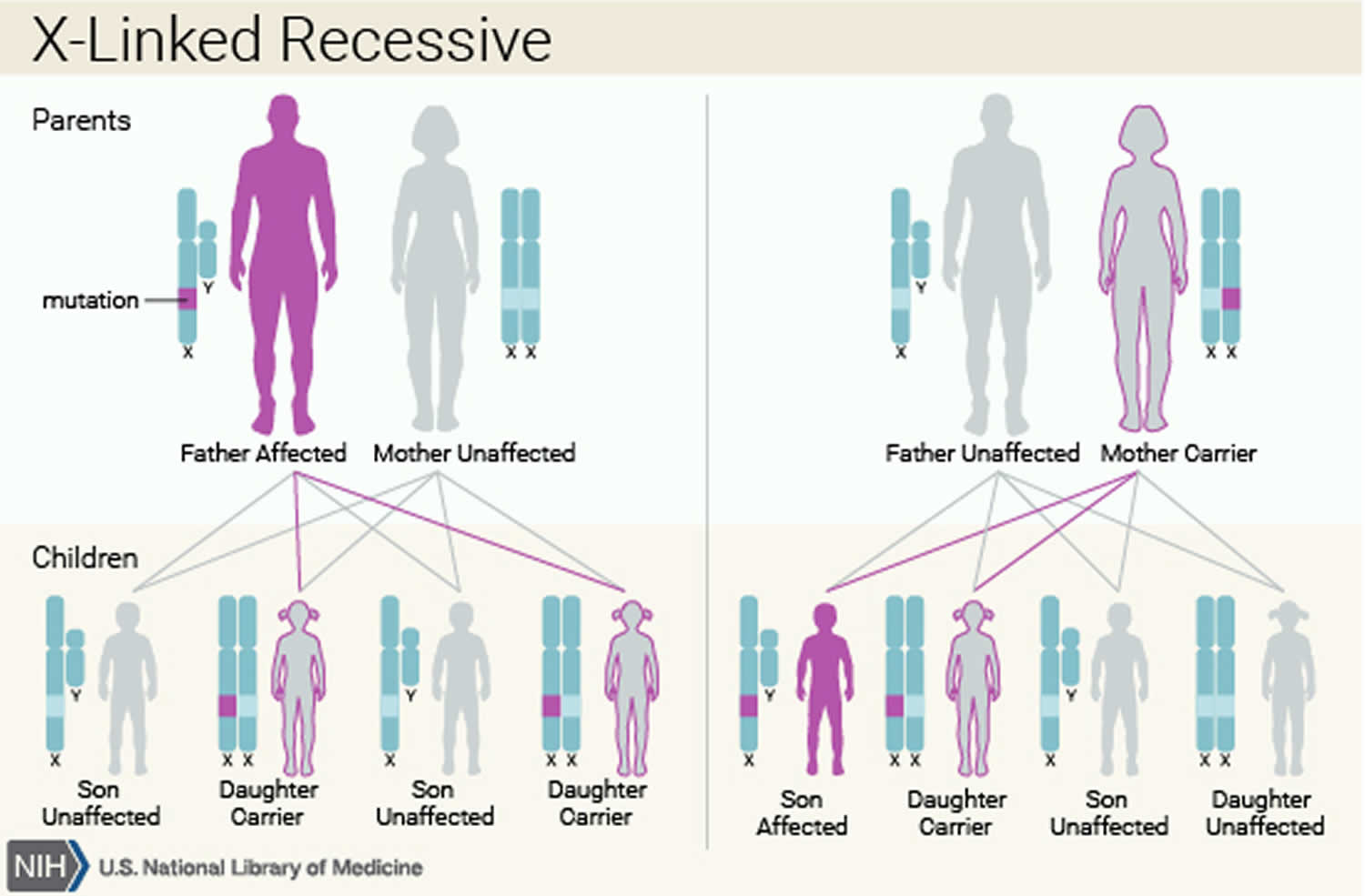
X-linked recessive disorders are conditions that are coded on the X chromosome. Females have two X chromosomes; males have one X chromosome and one Y chromosome. Therefore, in females, the normal gene on one X chromosome can mask disease traits on the other X chromosome. Since males have only one X chromosome, if they inherit the gene for a disease present on the X they will express the disease. Men with X-linked disorders transmit the gene to all their daughters, who are carriers, but never to their sons. Women who are carriers of an X-linked disorder have a 50 percent chance of transmitting the carrier condition to their daughters and a 50 percent risk of transmitting the disease to their sons.
X-linked ichthyosis can be diagnosed before birth by amniocentesis or chorionic villus sampling. Low maternal estriol levels can suggest the presence of X-linked ichthyosis.
X-linked ichthyosis is treated by applying skin softening creams and lotions. This can be especially effective after bathing while the skin is still moist. X-linked ichthyosis responds relatively well to topical treatment with alpha-hydroxy acids, which accelerate the shedding of the dead skin cells. Cholesterol containing emollients may also improve the scaling. Alpha-hydroxy acids may sting the skin of babies and young children and should be used cautiously or in combination with another mild emollient product.
What causes recessive X-linked ichthyosis?
Recessive X-linked ichthyosis is a disorder caused by a mutation of the enzyme steroid sulfatase (STS). Steroid sulfatase is involved in the metabolism of cholesterol sulphate in the skin. Steroid sulfatase deficiency leads to accumulation of cholesterol sulphate in the outer layer of the skin leading to a dysfunctional skin barrier and retention of the outer skin cells (corneocytes) causing the typical scaling.
X-linked ichthyosis is a rare disorder affecting one in 6,000 males 1.
The gene encoding steroid sulfatase has been mapped to the distal part of the X chromosome.
- 90% of patients with X-linked ichthyosis have complete deletions of this gene.
- The other cases include partial deletions or point mutations.
- Deletions can occur in the neighbouring genes causing a contiguous gene defect.
Therefore patients with X-linked ichthyosis should also be evaluated for the contiguous gene defect. Larger chromosomal deletions could result in:
- Kallmann syndrome
- Mental retardation
- X-linked recessive chondrodysplasia punctata
- Short stature.
X-linked ichthyosis inheritance pattern
The inheritance of X-linked ichthyosis is recessive because if the individual also has a normal STS gene, the condition is not expressed.
Females have two X-chromosomes and males have one. A male affected by X-linked ichthyosis passes the ichthyosis gene to his daughters via his X-chromosome. The daughters become carriers and usually have one affected gene and one normal gene. They can pass the abnormal gene to roughly half of their daughters and to half of their sons—who then manifest ichthyosis. Thus:
- Males are usually affected.
- Females are usually protected by their second X chromosome. They are carriers.
Approximately 1 in 6,000 males are affected by recessive X-linked ichthyosis, with no evident racial or geographical associations. There have been few cases reported in females. It is thought that these women have inherited the ichthyosis gene from both sides of the family.
Figure 1. X-linked recessive ichthyosis inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
X linked ichthyosis symptoms
Boys with X-linked ichthyosis appear normal at birth. The skin symptoms generally appear within the first year of life. Brownish scales that adhere to the skin are among the first signs of the disorder. The back and legs are most frequently involved early. The face, scalp, palms and soles, and hollows of the elbows and knees are usually spared.
In about half of adult males, comma-shaped corneal opacities occur in the eyes (seen on exam by an ophthalmologist), but they do not interfere with vision. Symptoms can improve markedly in the summer months and warm humid climates.
A small percentage of males may experience undescended testes (crytpchordism). These men may be at increased risk for contracting malignancies of the testes.
Women who are carriers of X-linked ichthyosis and give birth to sons with the disorder may experience a delay in labor or failure of labor to initiate. The enzyme defect can cause a decrease in production of maternal estriol in late pregnancy, which may affect labor and delivery. Low serum estriol levels detected by prenatal screening suggest the presence of a fetus with X-linked ichthyosis.
Recessive X-linked ichthyosis presents with prominent scaling.
- Scaling is usually distributed symmetrically.
- It is more evident on the extensor surfaces of the limbs and the side of the trunk.
- Scales can resemble fish scales; the brown or grey colour can lead to a ‘dirty appearance’.
- The face is usually free of scales except in the area in front of the ears (preauricular). Occasionally, flexures, neck and scalp are also affected.
- Scales on the scalp, neck and the preauricular areas tend to disappear during childhood.
- Palms and soles are very rarely involved.
- Hair and nails are normal.
- Typically desquamation improves during summer and deteriorates during dry and cold weather.
Non-skin manifestations of steroid sulfatase deficiency can occur as well.
- Due to low placental steroid sulfatase, pregnant mothers may suffer from prolonged labour when delivering affected infants.
- Corneal opacities can occur in affected males and female carriers.
- Undescended testicles (cryptorchidism) is found more commonly in men with x-linked ichthyosis than the general population.
- There is also an increased risk of testicular cancer, which is independent of the presence of testicular maldescent.
- Possible neurological involvement includes epilepsy, mental retardation and reduced ability to smell (hyposmia).
Involvement of the adjacent genes in patients with recessive x-linked ichthyosis can result in a variety of additional features.
X-linked ichthyosis diagnosis
Diagnosis is based mainly on history and clinical findings.
Biochemical analysis after birth on the placenta, skin fibroblasts and keratinocytes includes:
- Serum protein electrophoresis
- Steroid sulfatase activity assay.
Genetic analysis includes:
- Southern blot
- Fluorescent in situ hybridisation (FISH)
- Polymerase chain reaction (PCR).
Genetic analyses have missed a few cases of x-linked ichthyosis caused by point mutations.
Pre-natal diagnostic tests for X-linked ichthyosis include:
- Decreased estrogen levels in maternal urine
- Presence of non-hydrolyzed sulfate steroids in maternal urine
- Genetic analysis on chorionic villi or amniotic fluid samples, if the family history of STS gene defect is known.
Skin biopsy is usually not useful in confirming the disease as the epidermal microscopic findings may be subtle. They may include:
- Hyperkeratosis
- Hypergranulosis.
The genetic defect in X-linked ichthyosis results in a deficiency of the enzyme, steroid sulfatase. Genetic testing can detect the abnormality prenatally using amniocentesis or chorionic villus sampling (CVS). Decreased maternal serum or urine estriol levels and dehydroepiandrosterone levels can suggest X-linked ichthyosis in the fetus. Deficiency of the sulfatase enzyme in the placenta may result in failure of labor to initiate or progress.
X-linked ichthyosis is carried on the X sex chromosome. Women are unaffected but can carry the disease and pass it on to their sons. Men who have X-linked ichthyosis will have unaffected sons (they get their X chromosome from their mother), but their daughters will all be carriers. (For more information on the genetics of X-linked ichthyosis, refer to the Foundation’s publication, Ichthyosis, The Genetics of its Inheritance).
Approximately 50% of adult males and some female carriers will have asymptomatic comma-shaped corneal opacities (cloudy spots), which do not affect sight. Female carriers of X-linked ichthyosis occasionally report dry skin problems and, rarely, shadows of scales on the skin.
Results of genetic tests, even when they identify a specific mutation, can rarely tell you how mild or how severe a condition will be in any particular individual. There may be a general presentation in a family or consistent findings for a particular diagnosis, but it’s important to know that every individual is different. The result of a genetic test may be “negative,” meaning no mutation was identified. This may help the doctor exclude certain diagnoses, although sometimes it can be unsatisfying to the patient. “Inconclusive” results occur occasionally, and this reflects the limitation in our knowledge and techniques for doing the test.
X linked ichthyosis treatment
There is no definitive treatment for x-linked ichthyosis and current evidence is limited. High power studies for the treatments are lacking.
The aim of treatment is to improve the scaling of the skin and to improve the appearance of the skin. In some patients, treatment might not be required. Options include:
- Rubbing with a pumice stone or exfoliating sponge to remove scale
- Emollients applied after the bath to moisturise the skin
- Topical keratolytics containing lactic acid, glycolic acid, salicylic acid and urea; these agents can help with the desquamation and improve the appearance of the skin
- Topical isotretinoin
- Topical tazarotene 0.05% gel (receptor-selective retinoid)
- Calcipotriol ointment less than 100 g/week and liarozole 5% cream (not yet commercially available)
- Oral acitretin; its use is limited due to teratogenicity and adverse effects
- Oral liarozole (a retinoic acid metabolism blocking agent, not yet commercially available)
Genetic counseling can be also offered to patients and their families for further information regarding x-linked ichthyosis and inheritance pattern.
Research is ongoing to see whether patients can be treated with gene transfer.
Males should be advised to perform regular testicular self-examinations.
X linked ichthyosis prognosis
Recessive X-linked ichthyosis is a chronic condition and the disease persists through adult life.
- Scaling may improve over time.
- Life expectancy is normal.





{kind=link}