
What is casein
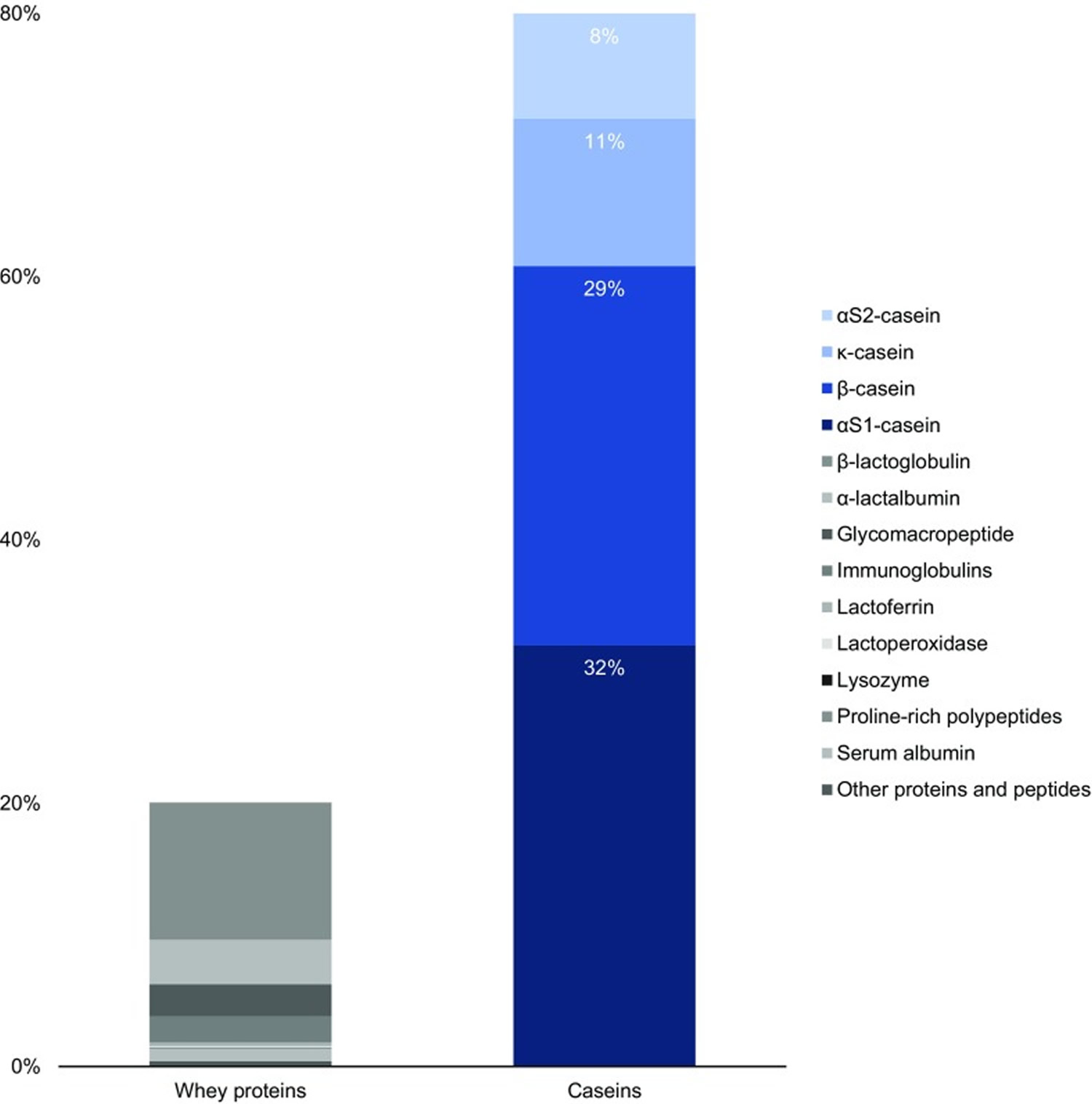
Casein is the collective name for a family of milk proteins. Caseins, in contrast to the second milk protein fraction, i.e. whey proteins, are insoluble and account for 80 % of total bovine milk proteins 1, which translates to 2.75 % of total milk components (Figure 1). Caseins, representing about 80% of the protein content in cow’s milk, are isolated from milk by acid or by rennet precipitation. The acid or isoelectric, precipitation is performed at pH 4.6, where the caseins precipitate and the whey proteins remain soluble. Caseins are flexible and heat stable proteins.
In bovine milk, casein comprises four peptides: αS1 casein (40%), αS2 casein (10%), β casein (36%) and κ casein (14%) differing in their amino acid, phosphorus and carbohydrate content but similar in their amphiphilic (having both hydrophilic and hydrophobic parts) character.
Milk proteins have long been known for their nutritional and technological value. Proteins are important constituents of the human diet, since they comprise a principal source of nitrogen and essential amino acids. Milk proteins have high nutritional value compared to other proteins because of their relatively high content of essential amino acids and good digestibility 2. This has led to the use of cow’s milk proteins as an essential ingredient in the manufacturing of specialized foods in the pharmaceutical and food industries 3.
Beta-casein has consistently demonstrated important biological activities on immune, cardiovascular, gastrointestinal and central nervous systems 4. Beta-casein is the second most abundant protein in cow’s milk representing 30% of total protein 5 . It is encoded by the CSN2 gene mapped on chromosome 6q31 and consists of 209-amino-acid single polypeptide chain, and molecular mass of about 24 kDa 6.
Beta-casein proteins may be present as one of two major genetic variants: A1 and A2 7. The distinguishing structure between these 2 forms of β-casein is the presence of either histidine (His67) in A1 or proline (Pro67) in A2 at position 67 of this 209–amino acid protein, with A1 being consequential to a point mutation from Pro67 to His67 occurring in ancestors to modern European-type cattle 8. A2 beta-casein is recognized as the original beta-casein variant because it existed before a proline67 to histidine67 point mutation caused the appearance of A1 beta-casein in some European herds some 5000–10,000 years ago 9.
In human milk, beta-casein (~68% of total casein) is of the A2 type, with a proline at the equivalent position on the beta-casein protein chain 10. Human bioactive opioid peptide beta-casomorphin-7 (BCM-7) has a different amino acid sequence to bovine bioactive opioid peptide beta-casomorphin-7 (BCM-7), with homology in five of seven amino acids (differing amino acids at positions four and five) 11 and considerably weaker opioid activity 12. Wada and Lonnerdal 11 examined non-digested and in vitro-digested human milk, and reported the presence of human BCM-9 (which has a proline at position eight), but not human BCM-7 or BCM-5 (i.e., BCM-5 is the truncated form of BCM-7). However, Jarmolowska et al. reported the presence of both human BCM-5 and BCM-7 in colostrum (averaging 5 and 3 μg/mL respectively), but at 2 months into the lactation period, the authors reported much lower quantities 13. It has been postulated that casomorphin functionality in neonates may relate to maternal bonding, gastrointestinal function, mucosal development and sleep induction 13.
Figure 1. Standard protein content in bovine milk
A1 beta-casein has only been found in cattle of European origin. Purebred Asian and African cattle produce milk containing only the A2 beta-casein type, although some cattle presenting phenotypically as Asian or African cattle may produce A1 beta-casein as a consequence of crossbred ancestry. The relative prevalence of A1 and A2 beta-casein in cattle is breed-dependent, with Northern European breeds generally having higher levels of A1 beta-casein than Southern European breeds. Guernsey and Fleckvieh breeds are generally considered to have a particularly high A2 allele frequency. However, within any specific herd, basing the estimation of allele frequency on breed category is not reliable. In the herds in many Western countries, the ratio of A1:A2 is approximately 1:1 14. Herd testing for beta-casein alleles can be undertaken using DNA analysis, which is available commercially in some countries. Converting a specific herd by selective breeding to eliminate all A1 beta-casein from the milk can be achieved within 4 years using intensive methods of animal selection that incorporate the use of sex-selected semen, but more typically this will take 5–8 years or longer 15.
There is increasing evidence that A1 beta-casein, a protein produced by a major proportion of European-origin cattle but not purebred Asian or African cattle, is also associated with cows’ milk intolerance 16. In humans, digestion of bovine A1 beta-casein, but not the alternative A2 beta-casein, releases beta-casomorphin-7 (BCM-7), which activates μ-opioid receptors expressed throughout the gastrointestinal tract and body. Studies in rodents show that milk containing A1 beta-casein significantly increases gastrointestinal transit time, production of dipeptidyl peptidase-4 (DPP4) and the inflammatory marker myeloperoxidase compared with milk containing A2 beta-casein 16. Co-administration of the opioid receptor antagonist naloxone blocks the myeloperoxidase and gastrointestinal motility effects, indicating opioid signaling pathway involvement. In humans, a double-blind, randomized cross-over study showed that participants consuming A1 beta-casein type cows’ milk experienced statistically significantly higher Bristol stool values compared with those receiving A2 beta-casein milk. The Bristol stool scale, is a diagnostic medical tool designed to classify the form of human faeces into seven categories. It is used in both clinical and experimental fields. Additionally, a statistically significant positive association between abdominal pain and stool consistency was observed when participants consumed the A1 but not the A2 diet. However, further studies of the role of A1 beta-casein in milk intolerance are needed.
There is wide-ranging evidence for both inflammatory and immune responses to casomorphins within the gastrointestinal system. However, the overall implications of these responses are not fully understood. It has been shown in both rats 17 and mice 18 that A1 beta-casein is associated with increased levels of the inflammatory marker myeloperoxidase in the colon. This effect is eliminated by administration of naloxone, indicating that it is an opioid-dependent response. Interestingly, intestinal inflammation enhances the potency of μ-opioid receptor agonists in inhibiting gastrointestinal transit, and increases the expression of μ-opioid receptors in the mouse intestine 19. It has also been shown in rats that A1 beta-casein stimulates the production of the enzyme dipeptidyl peptidase 4 (DPP4) in the jejunum 17. However, this effect is not attenuated by naloxone administration, indicating a non-opioid effect of A1 beta-casein on DPP4. The full implications of this are not understood, but it is notable that DPP4 degrades the gut incretin hormones rapidly. In humans, incretin hormones modulate insulin and glucose metabolism 20 and affect antroduodenal motility 21. Dipeptidyl peptidase 4 (DPP4) inhibitors are now widely used in the management of type 2 diabetes mellitus.
The avoidance of A1 is feasible within dairy-based diets through the consumption of goat, sheep, and buffalo milk or through the consumption of bovine milk from the native Asian and African bovine breeds, or through the consumption of milk from genetically selected herds of European-type cattle that are certified free of the His67 mutation. Such herds are being developed in many countries. Bovine milk that is free of A1 is now available commercially in a range of countries, including Australia, the United Kingdom, the United States, New Zealand, and The Netherlands, and is widely promoted as beneficial for people who suffer from milk intolerances. Infant formula containing casein but free of A1 is now marketed widely in China and Australia and is promoted commercially as being more gentle on the infant digestive system.
Gastrointestinal Effects of A1 Compared with A2 Beta-Casein
Once milk or milk products are consumed, the action of digestive enzymes in the gut on A1 beta-casein releases the bioactive opioid peptide beta-casomorphin-7 (BCM-7) 22. In contrast, A2 beta-casein releases much less and probably minimal amounts of bioactive opioid peptide beta-casomorphin-7 (BCM-7) under normal gut conditions 14. However, it is notable that under specific in vitro conditions relating to pH and enzyme combinations not found in the human gut, A2 beta-casein can also release some bioactive opioid peptide beta-casomorphin-7 (BCM-7) 23.
Beta-casomorphins (β-casomorphins) are μ-opioid receptor ligands 24. The natural casomorphins of relevance are beta-casomorphin-5 (BCM-5), beta-casomorphin-7 (BCM-7) and beta-casomorphin-9 (BCM-9). The most potent of these natural opioids is BCM-5. In theory, BCM-5 could be released from BCM-7 within the human biological system by the human equivalent of the enzyme carboxypeptidase Y and there is some evidence supporting this 25. Wasilewska et al. reported that bovine BCM-5 is present in the serum of exclusively breastfed human babies whose mothers consumed bovine milk 25. However, it has not been demonstrated whether the BCM-5 was hydrolyzed from BCM-7 by the mothers and passed via their breastmilk to the infants, or whether the mothers passed bovine BCM-7 via their breastmilk to the infants where it was subsequently degraded to BCM-5 before or after intestinal absorption.
Rodent studies have consistently reported opioid-mediated reduction in the rate of gastric emptying and increases in gastrointestinal transit time after the consumption of commercial casein. In vivo assays in rodents showed that a casein meal slowed gastric emptying and increased gastrointestinal transit time, compared with a whey protein meal 26. Similarly, in dogs, decreased intestinal motility and motor activity were observed with a casein-rich meal compared with a soy protein meal 27. Casein has also been shown to slow gastrointestinal transit time in young rats compared with hydrolyzed casein that has been predigested and which does not release beta-casomorphins (β-casomorphins) 28. In each case, the effects of casein were reversed by naloxone.
In a direct comparison of A1 and A2 fed to Wistar rats, gastrointestinal transit time was significantly greater in the A1 group between 8 and 14 h postprandially 29. Co-administration of naloxone decreased gastrointestinal transit time significantly in the A1 diet group but not in the A2 diet group at 8 and 11 h, but not at 14 h.
There is also some evidence that BCM-7 may interact with κ-opioid receptors in the gut. When administered in combination with enterostatin, which acts on κ-opioid receptors, via a gastric cannula, BCM-7 partially reversed the decrease in fat intake from a high-fat diet, observed with enterostatin alone, but did not affect intake from a low-fat diet 30.
The in vivo release of bioactive opioid peptide beta-casomorphin-7 (BCM-7) from each liter of bovine milk will depend on the protein content of the milk (which is in turn affected by the breed, animal feeding and component standardization procedures during milk processing), the proportion of A1 and A2 beta-casein, and possibly the specific gastrointestinal conditions of the individual. There is now clear evidence that bioactive opioid peptide beta-casomorphin-7 (BCM-7) is released not only from milk but also from yogurt and cheese, and in all likelihood any milk product 31. There is also evidence that there is modest release of bioactive opioid peptide beta-casomorphin-7 (BCM-7) in the cheese- and yogurt-making processes, but that during the latter, certain bacteria present in yogurt may hydrolyze BCM-7 32. Whether such bacteria consumed in yogurt also have a similar influence within the human gastrointestinal tract is unknown.
Casein protein vs Whey protein
Casein protein
Caseins not only provide adequate amounts of essential amino acids, but peptides derived from caseins have been shown to express various biological effects. Bioactive peptides are produced by in vitro and in vivo enzymatic proteolysis of bovine and human caseins 33.
Casein derivatives were tested in treating dry mouth, dentin hypersensitivity and in caries prevention 34. In a randomized clinical trial with subjects with salivary gland dysfunction (radiotherapy and Sjögren’s syndrome patients) two mouthrinse solutions containing either casein derivatives with calcium phosphate or a 0.05% sodium fluoride (as control), used for 12 months, were compared 35. No statistically significant differences between the two groups regarding coronal caries were found. between the two.
Hydrolyzed casein was found effective in decreasing postprandial glucose concentrations in type 2 diabetes mellitus patients who continued their oral anti-diabetic medication 36. In a double-blind trial single meal replacements with proprietary casein hydrolysate (insuVidaTM; DSM Nutritional Products) alone or with addition of leucine, unhydrolyzed casein or placebo were used. Postprandial serum glucose, insulin and glucagon concentrations were measured after 4 h. The addition of leucine to casein hydrolysate caused the biggest increase in insulin (by 51.8%). All three treatments increased glucagon concentration compared to placebo. In addition, a single dose of casein hydrolysate with or without leucine significantly lowered plasma glucose content compared to placebo and intact casein. The results suggest a benefit of the studied nutrients in management of type 2 diabetes.
β-casein and its peptides, as well as αS-casein, possess antioxidant and antimicrobial activity 37. As yet, however, none of the above-mentioned peptides has been clinically tested.
Whey protein
From the nutritional point of view, milk whey proteins have been considered superior to casein in various aspects. They present amino acid profile superior to casein, being similar to human milk, is what recommends whey proteins for the formulation of humanized milk products for replacement of bovine milk in infant nutrition 38. Whey protein from cow’s milk is also a rich source of essential and branched chain amino acids 39. Some publications 40, 41 reported on important differential properties between caseins and the milk whey proteins. It was observed that the caseins undergo much lower digestion and absorption than the whey proteins.
Whey protein is composed of several bioactive fractions including glycomacropeptide, β-lactoglobulin, α-lactalbumin and lactoferrin, with multiple health benefits against cancer, infection and inflammation 42. Dietary lactalbumin was found to suppress hunger in humans 43, decrease weight gain and adiposity in rats 44, mice 45 and minipigs 46, and improve glucose tolerance in diabetic rats 47 and minipigs 46. Further, lactalbumin and milk protein comparably decrease weight and fat mass in calorie restricted human subjects 48. Dietary supplementation with lactoferrin has been reported to modulate gut microbiota, decrease weight gain, reduce hepatic lipidosis, and improve glucose tolerance in mice 49 and produce greater weight and fat loss in calorie restricted mice 50. Others reported that lactoferrin decreases hepatic lipid content and mesenteric fat without altering food intake, weight gain and body composition in mice 51. Similarly, in humans, lactoferrin supplementation for 8 weeks 52, but not 4 weeks 53, has been shown to decrease visceral adiposity in overweight subjects without altering caloric intake. The reduction in caloric intake with whey-based diets is associated with increased circulating concentrations of satiety hormones of the lower gut including glucagon-like peptide-1 (GLP-1) and peptide YY (PYY) in humans 54, and GLP-1 in rodents. Despite producing hypophagia, lactalbumin does not alter GLP-1 in humans 55. However, it is unknown whether whey fractions differentially modulate the secretion of these and other satiety hormones. Although, lactalbumin was found to transiently increase energy expenditure in exercising rats, such thermogenic effects are not observed in calorie restricted humans 48. Thus, despite some evidence for the effects of lactalbumin and lactoferrin on body weight, the relative efficacies of these whey fractions in modulating food intake, energy expenditure and gut hormone secretion, and whether these effects are independent of caloric intake, remain largely unknown.
In a study using diet induced obese rats 56, randomized to isocaloric diets: Control, Whey, Lactalbumin, Lactoferrin, or pair-fed to lactoferrin. Whey and lactalbumin produced transient hypophagia (suppression of caloric intake in animals), whereas lactoferrin caused prolonged hypophagia. Lactalbumin decreased weight and fat gain. Notably, lactoferrin produced sustained weight and fat loss, and attenuated the reduction in energy expenditure associated with calorie restriction. Lactalbumin and lactoferrin decreased plasma leptin and insulin, and lactalbumin increased peptide YY. Whey’s lactalbumin and lactoferrin improved glucose clearance partly through differential upregulation of glucoregulatory transcripts in the liver and skeletal muscle. Interestingly, lactalbumin and lactoferrin decreased hepatic lipidosis (disorder of lipid metabolism in the body tissues) partly through downregulation of lipogenic and/or upregulation of β-oxidation transcripts, and differentially modulated cecal bacterial populations. The findings of that study 56 demonstrated that protein quantity and quality are important for improving energy balance. Dietary lactalbumin and lactoferrin improved energy balance and metabolism, and decreased adiposity, with the effects of lactoferrin being partly independent of caloric intake.
Figure 2. Whey protein health benefits
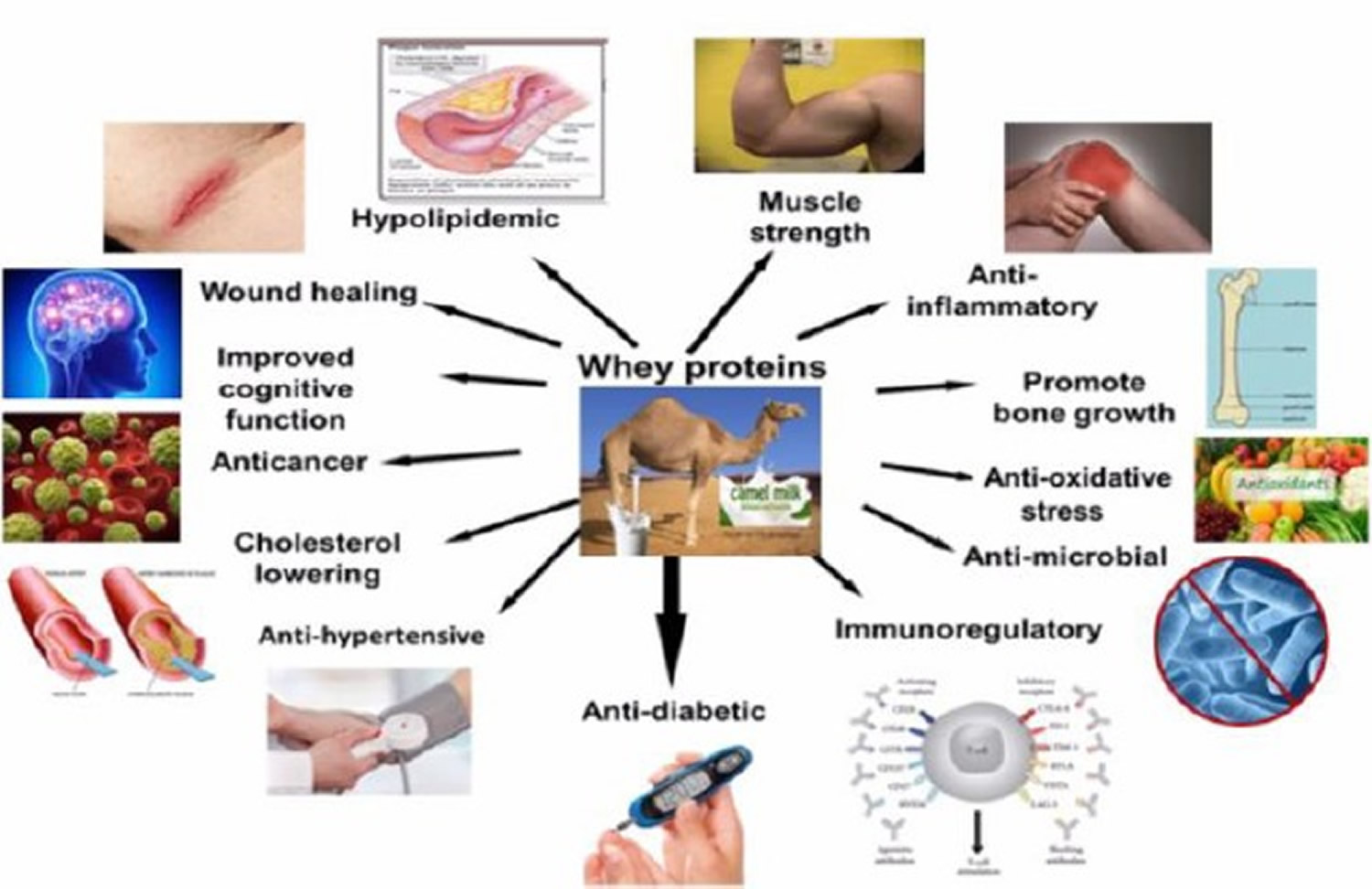
Table 1. Whey proteins component and their biological activities
| Components of whey protein | Biological Function | Species | References |
|---|---|---|---|
| α-lactalbumin | Enhancement of antibody response to systematic antigen stimulation and used in manufacturing of infant food | Camel, bovine, and human | 57 |
| Lactoferrin | Antimicrobial activities against microorganisms, anticancer, anti- inflammatory | Camel, bovine, and human | 58 |
| β-lactoglobulin | Source of essential and branched chain amino acid, responsible for child allergy | Bovine, buffalo, caprine, and equine | 59 |
| Lysozymes | Antibacterial protein present in milk, tears, and saliva, and thus plays an important role in enhancing innate immunity | Camel and bovine | 60 |
| Immunoglobulin | Enhances immune functions | Camel, bovine, and human | 61 |
| Lactoperoxidase | Suppression of bacterial growth | Camel and bovine | 62 |
| Glycomacropeptide | Has an inhibitory effect on acid gastric secretion and modifies the concentration of blood which regulates digestive peptides | Camel and bovine | 63 |
Milk Allergy
People who are allergic to cow’s milk react to one or more of the proteins in it. Curd, the substance that forms chunks in sour milk, contains 80% of milk’s proteins, including several called caseins. Whey, the watery part of milk, holds the other 20%. A person may be allergic to proteins in either or both parts of milk.
Every time the person eats these proteins, the body thinks they are harmful invaders. The immune system responds by kicking into high gear to fend off the “invader.” This causes an allergic reaction, in which chemicals like histamine are released in the body.
The release of these chemicals can cause someone to have the following problems:
- wheezing
- trouble breathing
- coughing
- hoarseness
- throat tightness
- stomachache
- vomiting
- diarrhea
- itchy, watery, or swollen eyes
- hives
- red spots
- swelling
- a drop in blood pressure
Milk allergy is like most food allergy reactions: It usually happens within minutes to hours after eating foods that contain milk proteins.
Although it’s not common, milk allergies can cause a severe reaction called anaphylaxis. Anaphylaxis may begin with some of the same symptoms as a less severe reaction, but then quickly worsen. A person might have trouble breathing, feel lightheaded, or pass out. If it’s not treated, anaphylaxis can be life-threatening.
Children who do not have symptoms shortly after they have milk can have a different type of reaction that causes problems hours to days later, such as:
- loose stools (possibly with blood)
- vomiting or gagging
- refusal to eat
- irritability or colic
- skin rashes, like dermatitis
Milk allergy is often confused with lactose intolerance because people can have the same kinds of things happening to them (like stomach pains or bloating, for example) with both conditions. But they’re not related:
- Milk allergy is a problem involving the immune system.
- Lactose intolerance involves the digestive system (which doesn’t produce enough of the enzyme needed to break down the sugar in milk).
How Can Doctors Tell It’s a Milk Allergy ?
If your doctor suspects you might have a milk allergy, he or she will probably refer you to an allergist or allergy specialist for more testing. The allergy specialist will ask you questions — like how often you have the reaction, the time it takes between eating a particular food and the start of the symptoms, and whether any family members have allergies or conditions like eczema and asthma.
The allergy specialist may do a skin test on you. This involves placing liquid extracts of milk protein on your forearm or back, pricking the skin a tiny bit, and waiting to see if a reddish, raised spot forms, indicating an allergic reaction.
You may need to stop taking anti-allergy medications (such as over-the-counter antihistamines) or prescription medicine 5 to 7 days before the skin test because they can affect the results. Most cold medicines and some antidepressants also may affect skin testing. Check with the allergist’s office if you are unsure about what medications need to be stopped and for how long.
The doctor also might take a blood sample and send it to a lab, where it will be mixed with some of the suspected allergen and checked for IgE antibodies.
These types of tests are used for diagnosing what doctors call a fast-onset type of milk allergy. But for people whose allergic reactions to milk develop more slowly, skin and blood tests are not as helpful.
In these cases, doctors try to diagnose the person using a food challenge. The person is told not to eat or drink anything made with milk for a period of time — usually a few weeks. Then, during the challenge, the person eats foods containing milk under a doctor’s close supervision. If symptoms come back after eating milk products, it’s a pretty sure bet the person has a milk allergy.
How Milk Allergy is Treated
To treat a milk allergy, the person who is allergic needs to completely avoid any foods that contain milk or milk products.
Avoiding milk involves more than just leaving the cheese off your sandwich. If you are allergic to milk, you need to read food labels carefully and not eat anything that you’re not sure about. It’s a good idea to work with a registered dietitian to develop an eating plan that provides all the nutrients you need while avoiding things you can’t eat.
If you have a severe milk allergy — or any kind of serious allergy — your doctor may want you to carry a shot of epinephrine with you in case of an emergency. Epinephrine comes in an easy-to-carry container about the size of a large marker. It’s easy to use — your doctor will show you how.
If you accidentally eat something with milk in it and start having serious allergic symptoms — like swelling inside your mouth, chest pain, or difficulty breathing — give yourself the shot right away to counteract the reaction while you’re waiting for medical help. Always call for emergency help when using epinephrine. You should make sure your school and even good friends’ houses keep injectable epinephrine on hand, too.
Keeping epinephrine with you at all times should be just part of your action plan for living with a milk allergy. It’s also a good idea to carry an over-the-counter antihistamine, which can help ease allergy symptoms in some people. But antihistamines should be used in addition to the epinephrine, not as a replacement for the shot.
If you’ve had to take an epinephrine shot because of an allergic reaction, go immediately to a medical facility or hospital emergency room so they can give you additional treatment if you need it. Sometimes, anaphylactic reactions are followed by a second wave of symptoms a few hours later. So you might need to be watched in a clinic or hospital for 4 to 8 hours following the reaction.
Living With a Milk Allergy
It can be challenging to eliminate milk from your diet, but it’s not impossible. Because most people don’t get enough calcium in their diets even if they do drink milk, many other foods are now enriched with calcium, such as juices, cereals, and rice and soy beverages. But before you eat or drink anything calcium-enriched, make sure it’s also dairy-free.
Milk and milk products can lurk in strange places, such as processed lunchmeats, margarine, baked goods, artificial butter flavor, and non-dairy products. Chocolate is another product that may contain dairy — so be sure to check the label before you eat it.
Manufacturers of foods sold in the United States must list on their labels whether a food contains any of the most common allergens. This means that you should be able to find the word “milk” stated plainly in the ingredients list, in parentheses in the ingredients list, or somewhere on the label with a statement like: “Contains milk.”
It is optional, however, for food manufacturers to use “may contain” statements. The U.S. Food and Drug Administration does not control whether companies can say things like “Processed in a facility that also processes milk products” or “May contain milk.” So call the manufacturer to be sure if you see statements like this on a food label.
New labeling requirements make it a little easier than reading the ingredients list — instead of needing to know that the ingredient “hydrolyzed casein” comes from milk protein, you should be able to tell at a glance which foods to avoid. But it’s still a good idea to get to know the “code words” for milk products when you see them in the ingredients of a food.
Some ingredients and foods that contain milk are:
- casein, calcium casein, casein hydrolysate, magenesium casein, potassium casein, rennet casein, sodium casein
- dairy products like cheese, yogurt, milk, pudding, sour cream, and cottage cheese
- butter, butter flavoring (such as diacetyl), butter fat, butter oil, ghee
- lactalbumin, lactoalbumin phosphate, lactaglobulin, lactose, lactoferrin, lactulose
- non-dairy creamers
- whey, whey hydrolysate
Vegan foods are made without animal products, such as eggs or milk. You can buy vegan products at health food stores. Be careful to read the labels of soy cheeses, though. They may say “milk-free” but could contain milk protein.
For your sweet tooth, soy- or rice-based frozen desserts, sorbets, and puddings are good substitutes for ice cream (as long as you’re not allergic to soy), as are ice pops. For baking, milk substitutes work as well as milk and some come out better. Dairy-free margarine works as well as butter for recipes and spreading on your bagel.
Try to avoid fried foods or foods with batter on them. Even if the batter doesn’t contain milk products, the oil used to fry the foods may have been used to fry something that contains milk.
People are usually understanding when it comes to food allergies — nobody wants to risk your health. When dining out, tell the waitstaff about anything you’re allergic to. Order the simplest foods and ask the waitstaff detailed questions about menu items. At a friend’s house, explain your situation and don’t be embarrassed to ask questions if you’re staying for a meal.
Having a milk allergy doesn’t mean you can’t still enjoy eating. In fact, some people think that some of the milk substitutes — like vanilla soy milk — taste better than regular cow’s milk. As with any specialized diet, you’ll probably find that avoiding milk gives you the chance to explore and discover some great foods that you’d never have found otherwise.
Milk alternatives for infants
Some research suggests that breast-feeding during the first four to six months of a baby’s life instead of giving a standard cow’s milk formula can help prevent milk allergy. In children who are allergic to milk, breast-feeding and use of hypoallergenic formula can prevent allergic reactions.
Breast-feeding is the best source of nutrition for your child. Breast-feeding for at least the first four to six months of life if possible is recommended, especially if your infant is at high risk of developing a milk allergy.
Hypoallergenic formulas are produced by using enzymes to break down (hydrolyze) milk proteins, such as casein or whey. Further processing can include heat and filtering. Depending on the level of processing, products are classified as either partially or extensively hydrolyzed. Or they may also be called elemental formulas.
Some hypoallergenic formulas aren’t milk based, but instead contain amino acids. Besides extensively hydrolyzed products, amino-acid-based formulas are the least likely to cause an allergic reaction.
Soy-based formulas are based on soy protein instead of milk. Soy formulas are fortified to be nutritionally complete — but, unfortunately, some children with a milk allergy also develop an allergy to soy.
If you’re breast-feeding and your child has a milk allergy, cow’s milk proteins passed through your breast milk may cause an allergic reaction. Then you may need to exclude all products that contain milk from your diet. Talk to your doctor if you know — or suspect — your child has a milk allergy and develops allergy signs and symptoms after breast-feeding.
If you or your child is on a milk-free diet, your doctor or dietitian can help you plan nutritionally balanced meals. You or your child may need to take supplements to replace calcium and nutrients found in milk, such as vitamin D and riboflavin.
References- Milk nutritional composition and its role in human health. Pereira PC. Nutrition. 2014 Jun; 30(6):619-27. https://www.ncbi.nlm.nih.gov/pubmed/24800664/
- Hambraeus L. Nutritional Aspects of Milk Proteins. In: Fox PF, editor. Advanced Dairy Chemistry–1: Proteins. London: Elsevier Applied Science; 1992. pp. 457–490.
- Mulvihill D.M., Ennis M.P. Functional milk proteins: Production and utilization. In: Fox P.F., McSweeney P.L.H., editors. Advanced Dairy Chemistry Proteins. 3rd ed. Volume 1. Springer International Publishing AG; New York, NY, USA: 2003. pp. 1175–1228.
- Raies M.H., Kapila R., Shandilya U.K., Kapila S. Impact of milk derived β-casomorphins on physiological functions and trends in research: A review. Int. J. Food Prop. 2014;17:1726–1741.
- Phelan M., Aherne A., FitzGerald R.J., O’Brien N.M. Casein-derived bioactive peptides: Biological effects, industrial uses, safety aspects and regulatory status. Int. Dairy J. 2009;19:643–654. doi: 10.1016/j.idairyj.2009.06.001.
- Swaisgood H.E. Chemistry of the caseins. In: Fox P.F, editor. Advanced Dairy Chemistry. 1st ed. Volume 1. Elsevier Applied Science; London, UK: 1992. pp. 63–110.
- Formaggioni P., Summer A., Malacarne M., Mariani P. Milk protein polymorphism: Detection and diffusion of the genetic variants in Bos genus. Ann. Fac. Med. Vet. Univ. Parma. 1999;19:127–165.
- Kamiński S, Cieslińska A, Kostyra E. Polymorphism of bovine beta-casein and its potential effect on human health. J Appl Genet 2007;48:189–98. https://www.ncbi.nlm.nih.gov/pubmed/17666771
- Ng-Kwai-Hang K.F., Grosclaude F. Genetic polymorphism of milk proteins. In: Fox P.F., McSweeney P.L.H., editors. Advanced Dairy Chemistry: Volume 1: Proteins, Parts A & B. Kluwer Academic/Plenum Publishers; New York, NY, USA: 2002. pp. 739–816.
- Hamosh M., Hong H., Hamosh P. Beta-Casomorphins: Milk-β-casein derived opioid peptides. In: Lebenthal E., editor. Textbook of Gastroenterology and Nutrition in Infancy. 2nd ed. Raven Press; New York, NY, USA: 1989. pp. 143–150.
- Bioactive peptides released from in vitro digestion of human milk with or without pasteurization. Wada Y, Lönnerdal B. Pediatr Res. 2015 Apr; 77(4):546-53. https://www.ncbi.nlm.nih.gov/pubmed/25580741/
- Novel opioid peptides derived from human beta-casein: human beta-casomorphins. Brantl V. Eur J Pharmacol. 1984 Oct 30; 106(1):213-4. https://www.ncbi.nlm.nih.gov/pubmed/6529969/
- Changes of beta-casomorphin content in human milk during lactation. Jarmołowska B, Sidor K, Iwan M, Bielikowicz K, Kaczmarski M, Kostyra E, Kostyra H. Peptides. 2007 Oct; 28(10):1982-6. https://www.ncbi.nlm.nih.gov/pubmed/17869380/
- De Noni R.J., FitzGerald H.J.T., Korhonen Y., Le Roux C.T., Livesey I., Thorsdottir D., Tomé R.W. Scientific Report of EFSA prepared by a DATEX Working Group on the potential health impact of β-casomorphins and related peptides. EFSA Sci. Rep. 2009;231:1–107.
- Mencarini I.R., Woodford K.B., Old K.M. Comparing herd selection strategies for A2 beta-casein. Proc. N. Z. Soc. Anim. Prod. 2013;73:149–154.
- Pal S, Woodford K, Kukuljan S, Ho S. Milk Intolerance, Beta-Casein and Lactose. Nutrients. 2015;7(9):7285-7297. doi:10.3390/nu7095339. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586534/
- Barnett M.P., McNabb W.C., Roy N.C., Woodford K.B., Clarke A.J. Dietary A1 β-casein affects gastrointestinal transit time, dipeptidyl peptidase-4 activity, and inflammatory status relative to A2 β-casein in Wistar rats. Int. J. Food Sci. Nutr. 2014;65:720–727. doi: 10.3109/09637486.2014.898260. https://www.ncbi.nlm.nih.gov/pubmed/24649921
- Ul Haq M.R., Kapila R., Sharma R., Saliganti V., Kapila S. Comparative evaluation of cow β-casein variants (A1/A2) consumption on Th2-mediated inflammatory response in mouse gut. Eur. J. Nutr. 2014;53:1039–1049. doi: 10.1007/s00394-013-0606-7. https://www.ncbi.nlm.nih.gov/pubmed/24166511
- Pol O, Sasaki M, Jiménez N, Dawson VL, Dawson TM, Puig MM. The involvement of nitric oxide in the enhanced expression of μ-opioid receptors during intestinal inflammation in mice. British Journal of Pharmacology. 2005;145(6):758-766. doi:10.1038/sj.bjp.0706227. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1576189/
- Holst J.J., Gromada J. Role of incretin hormones in the regulation of insulin secretion in diabetic and nondiabetic humans. Am. J. Physiol. Endocrinol. Metab. 2004;287:E199–E206. doi: 10.1152/ajpendo.00545.2003. http://ajpendo.physiology.org/content/287/2/E199.long
- Schirra J, Nicolaus M, Roggel R, et al. Endogenous glucagon‐like peptide 1 controls endocrine pancreatic secretion and antro‐pyloro‐duodenal motility in humans. Gut. 2006;55(2):243-251. doi:10.1136/gut.2004.059741. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1856508/
- Release of β-casomorphin-7/5 during simulated gastrointestinal digestion of milk β-casein variants from Indian crossbred cattle (Karan Fries). Ul Haq MR, Kapila R, Kapila S. Food Chem. 2015 Feb 1; 168():70-9. https://www.ncbi.nlm.nih.gov/pubmed/25172685/
- Milk from cows of different β-casein genotypes as a source of β-casomorphin-7. Cieślińska A, Kostyra E, Kostyra H, Oleński K, Fiedorowicz E, Kamiński S. Int J Food Sci Nutr. 2012 Jun; 63(4):426-30. https://www.ncbi.nlm.nih.gov/pubmed/22080615/
- Opioid activities of beta-casomorphins. Brantl V, Teschemacher H, Bläsig J, Henschen A, Lottspeich F. Life Sci. 1981 Apr 27; 28(17):1903-9. https://www.ncbi.nlm.nih.gov/pubmed/6265721/
- Cow’s-milk-induced infant apnoea with increased serum content of bovine β-casomorphin-5. Wasilewska J, Kaczmarski M, Kostyra E, Iwan M. J Pediatr Gastroenterol Nutr. 2011 Jun; 52(6):772-5. https://www.ncbi.nlm.nih.gov/pubmed/21478761/
- Daniel H, Vohwinkel M, Rehner G. Effect of casein and beta-casomorphins on gastrointestinal motility in rats. J Nutr 1990;120:252–7.
- Defilippi C, Gomez E, Charlin V, Silva C. Inhibition of small intestinal motility by casein: a role of beta casomorphins? Nutrition 1995;11:751–4.
- Mihatsch WA, Franz AR, Kuhnt B, Hogel J, Pohlandt F. Hydrolysis of casein accelerates gastrointestinal transit via reduction of opioid receptor agonists released from casein in rats. Biol Neonate 2005;87:160–3.
- Barnett MP, McNabb WC, Roy NC, Woodford KB, Clarke AJ. Dietary A1 beta-casein affects gastrointestinal transit time, dipeptidyl peptidase-4 activity, and inflammatory status relative to A2 beta-casein in Wistar rats. Int J Food Sci Nutr 2014;65:720–7.
- White CL, Bray GA, York DA. Intragastric beta-casomorphin(1–7) attenuates the suppression of fat intake by enterostatin. Peptides 2000;21:1377–81.
- Release of β-casomorphins 5 and 7 during simulated gastro-intestinal digestion of bovine β-casein variants and milk-based infant formulas. Noni ID. Food Chem. 2008 Oct 15; 110(4):897-903. https://www.ncbi.nlm.nih.gov/pubmed/26047276/
- Enzymatic ability of Bifidobacterium animalis subsp. lactis to hydrolyze milk proteins: identification and characterization of endopeptidase O. Janer C, Arigoni F, Lee BH, Peláez C, Requena T. Appl Environ Microbiol. 2005 Dec; 71(12):8460-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1317388/
- Shah N.P.: Effects of milk-derived bioactives: an overview. Br. J. Nutr., 2000; 84: S3-S10
- Azarpazhooh A., Limeback H.: Clinical efficacy of casein derivatives: a systematic review of the literature. J. Am. Dent. Assoc., 2008; 139: 915-924.
- Hay K.D., Thomson W.M.: A clinical trial of the anticaries efficacy of casein derivatives complexed with calcium phosphate in patients with salivary gland dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod., 2002; 93: 271-275
- Geerts B.F., van Dongen M.G., Flameling B., Moerland M.M., de Kam M.L., Cohen A.F., Romijn J.A., Gerhardt C.C, Kloek J., Burggraaf J.: Hydrolyzed casein decreases postprandial glucose concentrations in T2DM patients irrespective of leucine content. J. Diet. Suppl., 2011; 8: 280-292
- Darewicz M., Dziuba B., Minkiewicz P., Dziuba J.: The preventive potential of milk and colostrum proteins and protein fragments. Food Rev. Int., 2011; 27: 357-388.
- Hambraeus L. Nutritional Aspects of Milk Proteins. In: Fox PF, editor. Developments in Dairy Chemistry–1: Proteins. London: Applied Science Publishers; 1982. pp. 289–313.
- Piccolomini AF, Kubow S, Lands LC. Clinical Potential of Hyperbaric Pressure-Treated Whey Protein. Samman S, Darnton-Hill I, eds. Healthcare. 2015;3(2):452-465. doi:10.3390/healthcare3020452. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4939533/
- Boirie Y, Dangin M, Gachon P, Vasson M-P, Maubois J-L, Beaufrère B. Slow and fast dietary proteins differently modulate postprandial protein accretion. Proceedings of the National Academy of Sciences of the United States of America. 1997;94(26):14930-14935. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC25140/
- Protein metabolism. Slow and fast dietary proteins. Frühbeck G. Nature. 1998 Feb 26; 391(6670):843, 845. https://www.ncbi.nlm.nih.gov/pubmed/9495333/
- Emerging health properties of whey proteins and their clinical implications. Krissansen GW. J Am Coll Nutr. 2007 Dec; 26(6):713S-23S. https://www.ncbi.nlm.nih.gov/pubmed/18187438/
- Krissansen GW. Emerging health properties of whey proteins and their clinical implications. J. Am. Coll. Nutr. 2007;26(6):713S–23S. doi: 10.1080/07315724.2007.10719652. https://www.ncbi.nlm.nih.gov/pubmed/18187438
- Hamad EM, Taha SH, Abou Dawood AG, Sitohy MZ, Abdel-Hamid M. Protective effect of whey proteins against nonalcoholic fatty liver in rats. Lipids Health Dis. 2011;10 doi: 10.1186/1476-511X-10-57 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096574/
- Tauriainen E, et al. Skeletal muscle gene expression profile is modified by dietary protein source and calcium during energy restriction. J. Nutrigenet. Nutrigenomics. 2011;4(1):49–62. doi: 10.1159/000327132. https://www.ncbi.nlm.nih.gov/pubmed/21525773
- Blat S, et al. Dietary alpha-lactalbumin supplementation alleviates normocaloric western diet-induced glucose intolerance in Gottingen minipigs. Obesity. 2015;23(2):415–21. doi: 10.1002/oby.20990. https://www.ncbi.nlm.nih.gov/pubmed/25594308
- Yamaguchi M, Takai S. Chronic administration of bovine milk-derived alpha-lactalbumin improves glucose tolerance via enhancement of adiponectin in Goto-Kakizaki rats with type 2 diabetes. Biol. Pharm. Bull. 2014;37(3):404–8. doi: 10.1248/bpb.b13-00762. https://www.ncbi.nlm.nih.gov/pubmed/24583859
- Soenen S, Hochstenbach-Waelen A, Westerterp-Plantenga MS. Efficacy of alpha-lactalbumin and milk protein on weight loss and body composition during energy restriction. Obesity. 2011;19(2):370–9. doi: 10.1038/oby.2010.146. https://www.ncbi.nlm.nih.gov/pubmed/20577225
- Sun J, Ren F, Xiong L, Zhao L, Gao H. Bovine lactoferrin suppresses high-fat diet induced obesity and modulates gut microbiota in C57BL/6J mice. J. Funct. Foods. 2016;22:189–200. doi: 10.1016/j.jff.2016.01.022.
- Shi J, et al. Metabolic effects of lactoferrin during energy restriction and weight regain in diet induced obese mice. J. Funct. Foods. 2012;4(1):66–78. doi: 10.1016/j.jff.2011.08.001.
- Morishita S, et al. Bovine lactoferrin reduces visceral fat and liver triglycerides in ICR mice. J. Oleo. Sci. 2013;62(2):97–103. doi: 10.5650/jos.62.97. https://www.ncbi.nlm.nih.gov/pubmed/23391533
- Ono T, et al. Potent anti-obesity effect of enteric-coated lactoferrin: decrease in visceral fat accumulation in Japanese men and women with abdominal obesity after 8-week administration of enteric-coated lactoferrin tablets. Br. J. Nutr. 2010;104(11):1688–95. doi: 10.1017/S0007114510002734. https://www.ncbi.nlm.nih.gov/pubmed/20691130
- Cox AJ, et al. Effects of short-term supplementation with bovine lactoferrin and/or immunoglobulins on body mass and metabolic measures: a randomised controlled trial. Int. J. Food Sci. Nutr. 2017;68(2):219–226. doi: 10.1080/09637486.2016.1224230. https://www.ncbi.nlm.nih.gov/pubmed/27592680
- Chungchunlam SM, Henare SJ, Ganesh S, Moughan PJ. Dietary whey protein influences plasma satiety-related hormones and plasma amino acids in normal-weight adult women. Eur. J. Clin. Nutr. 2015;69(2):179–86. doi: 10.1038/ejcn.2014.266. https://www.ncbi.nlm.nih.gov/pubmed/25563737
- Veldhorst MA, et al. A breakfast with alpha-lactalbumin, gelatin, or gelatin + TRP lowers energy intake at lunch compared with a breakfast with casein, soy, whey, or whey-GMP. Clin. Nutr. 2009;28(2):147–55. doi: 10.1016/j.clnu.2008.12.003. https://www.ncbi.nlm.nih.gov/pubmed/19185957
- Zapata RC, Singh A, Pezeshki A, Nibber T, Chelikani PK. Whey Protein Components – Lactalbumin and Lactoferrin – Improve Energy Balance and Metabolism. Scientific Reports. 2017;7:9917. doi:10.1038/s41598-017-09781-2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5577213
- Bounous G, Batist G, Gold P. Immunoenhancing property of dietary whey protein in mice:Role of glutathione. Clin Invest Med. 1989;12:154–161. https://www.ncbi.nlm.nih.gov/pubmed/2743633
- Legrand D, Pierce A, Elass E, Carpentier M, Mariller C, Mazurier J. Lactoferrin structure and functions. In Bioactive components of milk. Springer; 2008. pp. 163–194.
- Guimont C, Marchall E, Girardet JM, Linden G. Biologically active factors in bovine milk and dairy byproducts: Influence on cell culture. Crit RevFoodSci Nut. 1997;37:393–410. https://www.ncbi.nlm.nih.gov/pubmed/9227891
- El-Agamy EI, Nawar M, Shamsia SM, Awad S, Haenlein GF. Are camel milk proteins convenient to the nutrition of cow milk allergic children?Small Rumin Res. 2009;82:1–6.
- Laleye L, Jobe B, Wasesa A. Comparative study on heat stability and functionality of camel and bovine milk whey proteins. JDairySci. 2008;91:4527–4534. https://www.ncbi.nlm.nih.gov/pubmed/19038927
- Konuspayeva G, Faye B, Loiseau G, Levieux D. Lactoferrin and immunoglobulin contents in camel’s milk (camelus bactrianus, camelus dromedarius, and hybrids) from kazakhstan. J Dairy Sci. 2007;90:38–46. https://www.ncbi.nlm.nih.gov/pubmed/17183073
- El-Hatmi H, Girardet JM, Gaillard JL, Yahyaoui MH, Attia H. Characterisation of whey proteins of camel (camelus dromedarius) milk and colostrum. SmallRumin Res. 2007;70:267–271.
- Badr G, Ramadan NK, Sayed LH, Badr BM, Omar HM, Selamoglu Z. Why whey? Camel whey protein as a new dietary approach to the management of free radicals and for the treatment of different health disorders. Iranian Journal of Basic Medical Sciences. 2017;20(4):338-349. doi:10.22038/IJBMS.2017.8573. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5425915/





{kind=link}